You might be meeting every deadline, showing up for family, and keeping your schedule full while feeling empty inside.
That disconnect between outward success and inner struggle is what many people call high functioning depression, though it’s not a formal diagnosis.
The real difference lies in how depression shows up: major depressive disorder typically involves intense episodes lasting at least two weeks with clear impairment, while high functioning depression usually describes chronic, lower grade symptoms that persist for years while you continue to appear productive.
This article will clarify the diagnostic distinctions, symptom patterns, and why both deserve serious attention.
What is Major Depression?
Major depressive disorder is a formally recognized mood disorder defined by specific criteria in the DSM-5. According to diagnostic standards, MDD requires at least five symptoms during the same two week period, including either depressed mood or loss of interest and pleasure.
These symptoms must represent a change from previous functioning and cause clinically significant distress or impairment in social, occupational, or other important areas.
The nine symptom domains include sad mood, insomnia or hypersomnia, guilt or worthlessness, low energy, decreased concentration, appetite changes, anhedonia, psychomotor changes, and suicidal thoughts.
Importantly, impairment does not need to occur in every domain simultaneously. You might still work while experiencing severe social withdrawal, or maintain parenting responsibilities while losing all pleasure in life.
Major depression is episodic by nature. Episodes may be isolated or recurrent, and they can range from mild to severe.
Some people experience psychotic features during severe episodes. Between episodes, many people return to their previous baseline, though residual symptoms and functional deficits can persist even after mood improves.
What is High Functioning Depression?
High functioning depression is not an official clinical diagnosis. Multiple sources confirm that this term describes people who appear to function well externally while experiencing significant depressive symptoms internally. You might hold down a job, maintain relationships, meet responsibilities, and appear composed to others while privately struggling with persistent low mood, fatigue, hopelessness, and emotional numbness.
The formal diagnosis most often associated with this presentation is persistent depressive disorder, previously called dysthymia.
PDD involves depressed mood most days for at least two years in adults, along with at least two additional symptoms such as poor appetite or overeating, insomnia or hypersomnia, low energy, low self esteem, poor concentration, and hopelessness.
Unlike major depression’s episodic structure, PDD represents a chronic depressive baseline with no symptom free interval longer than two months.
The phrase “high functioning depression” captures a real phenomenon but can be misleading. It privileges external appearance over internal suffering and may delay diagnosis.
When clinicians, families, or patients believe depression must look visibly incapacitating, serious illness gets missed.
Core Differences Between the Two
Diagnostic Status and Duration
Major depression is a formal DSM and ICD diagnosis centered on threshold level symptom clusters lasting at least two weeks.
High functioning depression is an informal descriptor, not a diagnostic category. When it corresponds to a formal diagnosis, that diagnosis is usually persistent depressive disorder requiring at least two years of symptoms in adults.
This duration difference matters clinically. Major depression is typically episodic, with periods of illness followed by potential recovery.
PDD involves chronic symptoms that may fluctuate but rarely resolve completely. Some people experience both simultaneously, a pattern called double depression, where major depressive episodes are superimposed on an already chronic depressive baseline.
Symptom Intensity and Visibility
Major depression usually involves higher acute symptom intensity. During a major depressive episode, symptoms often become difficult to hide.
Profound anhedonia, severe fatigue, marked concentration failure, psychomotor slowing or agitation, and suicidal ideation may visibly interfere with daily tasks. Family, friends, and coworkers often notice tearfulness, withdrawal, slowed movement, or declining performance.
High functioning depression typically involves lower moment to moment symptom intensity but much longer duration.
The depressive burden is distributed over years rather than peaking in discrete episodes. Symptoms become normalized by the person and others. You might think “this is just my personality” or “I’m functioning, so it can’t be serious,” which delays recognition and treatment.
Functional Presentation Patterns
The most visible difference is how functioning appears. Major depression often disrupts observable role performance.
Work productivity declines, social withdrawal becomes obvious, self care deteriorates, and relationships suffer in ways others can see. The impairment is harder to conceal during acute episodes.
High functioning depression often preserves outward role performance. You continue working, parenting, socializing, and meeting obligations while experiencing substantial internal distress. This does not mean there is no impairment.
Rather, the impairment may be less obvious, partially compensated, or concentrated in subjective quality of life rather than gross role failure.
Research shows that functional impairment in PDD can be as severe as or more severe than in major depression.
The chronic nature of dysthymia can cause greater long term impairment than acute depression, with reduced likelihood of full time work and more interference with social activities. Preserved appearance of functioning does not equal low disability burden.
Symptom Overlap and Distinctions
Both conditions share extensive symptom overlap. Common symptoms include:
- Persistent sadness or low mood
- Loss of interest or pleasure in activities
- Fatigue and low energy
- Sleep disturbance
- Appetite or weight changes
- Difficulty concentrating or making decisions
- Feelings of worthlessness or excessive guilt
- Hopelessness
- Irritability
- Social withdrawal
- Suicidal thoughts in some cases
The difference lies more in pattern than content. Major depression tends to emphasize more pronounced neurovegetative symptoms like sleep disturbance, appetite change, psychomotor changes, and stronger acute anhedonia.
High functioning depression or PDD more commonly emphasizes low self esteem, pessimism, chronic apathy, and persistent emotional flatness.
In high functioning presentations, you might continue hobbies and social events mechanically with little enjoyment, maintain your schedule while crashing privately, meet deadlines with disproportionate strain, or appear dependable while feeling internally ashamed.
The symptoms are real depressive symptoms occurring in people who retain sufficient external organization, motivation, fear of stigma, perfectionism, or role obligation to continue performing.
Can You Function With Major Depression?
Yes. A person can meet full criteria for major depressive disorder and still function in some or many areas of life.
DSM based diagnosis does not require total incapacity, only sufficient symptom burden plus clinically significant distress or impairment in one or more important domains. Impairment can be selective, hidden, or compensated.
Someone may still go to work, parent, attend school, and smile socially while experiencing significant decline in quality of functioning, increased error rates, emotional numbness, inability to enjoy life, chronic exhaustion, or suicidal ideation. An attorney may continue billing hours but become socially detached and suicidal.
A parent may care for children but be unable to experience pleasure, intimacy, or concentration. A student may keep grades up while suffering severe insomnia, hopelessness, and emotional collapse.
Functioning is domain specific, not all or nothing. You might maintain employment while experiencing severe social impairment, or meet family obligations while losing all capacity for joy. Visible productivity is a poor proxy for mental health.
Depression exists on a heterogeneous spectrum of presentation, and outward productivity does not rule out serious illness, meaningful impairment, or suicide risk.
Why High Functioning Depression Gets Missed?
Several factors contribute to underrecognition. First, stereotypes about depression focus on obvious incapacity: inability to get out of bed, visible tearfulness, complete withdrawal, and clear occupational collapse. When your depression does not match that image, you, your family, and even clinicians may miss it.
Second, chronic symptoms become normalized. When you have felt low, tired, joyless, and hopeless for years, it stops feeling like an illness and starts feeling like who you are. You may not recognize that your baseline is actually a depressive state requiring treatment.
Third, stigma and masking play major roles. Many people maintain a normal appearance and tell others they are fine, causing even themselves to miss the significance of their symptoms. Social stigma around mental illness drives concealment.
Perfectionism, achievement orientation, responsibility for others, and fear of judgment can all motivate continued performance despite internal suffering.
Fourth, some people cannot afford to stop functioning. Employment, caregiving, debt, and cultural expectations may force continued performance. Outward functioning under those pressures should not be misread as low severity.
Double Depression: When Both Occur Together?
A particularly important clinical pattern is double depression, where a person meets criteria for both persistent depressive disorder and major depressive disorder simultaneously.
This happens when a major depressive episode is superimposed on chronic depressive symptoms.
For example, you might have years of low mood, low self esteem, fatigue, hopelessness, and reduced joy while still maintaining work and daily responsibilities.
Then you experience a two month collapse with profound anhedonia, insomnia, weight loss, psychomotor slowing, suicidal ideation, and inability to work. That is not a switch from “not depressed” to “depressed.” It is PDD plus a superimposed MDD episode.
This pattern shows that high functioning depression and major depression are not mutually exclusive categories.
They may represent different syndromes in different people, different phases in one person, or overlapping layers in the same illness course. The contrast is real, but so is the overlap.
Severity: Acute Intensity vs Chronic Burden
A major depressive episode can be mild, moderate, or severe. In common clinical terms, MDD usually represents higher acute symptom burden.
Severe episodes can involve profound despair, inability to function normally, and obvious disability. This aligns with the common image of depression as visible collapse.
However, severity is not reducible to visible productivity. There are at least two kinds of severity relevant here: acute symptomatic severity and longitudinal burden severity. Major depression often wins on acute intensity.
But persistent depressive disorder may equal or exceed MDD in cumulative burden because it persists for years.
Research confirms that functional impairments in PDD can be as severe as or more severe than in major depression. The most clinically useful distinction is not “major depression is severe, high functioning depression is mild.”
The better conclusion is that major depression is usually more acutely severe, while high functioning depression is often more chronically entrenched and therefore can be equally or more disabling over time.
Suicide Risk in Both Conditions
Both major depression and persistent depressive disorder carry elevated suicide risk. Major depression is strongly associated with suicidal behavior, and thorough suicide assessment is recommended in depression care broadly. PDD also carries heightened risk of suicidal thoughts and behaviors.
The label “high functioning” can be dangerous if it minimizes risk. A person may be outwardly productive and still suicidal. Some sources suggest that smiling depression can be especially dangerous because individuals still have enough energy and organization to act on suicidal thoughts.
While that claim should be stated cautiously, the broader evidence certainly supports that suicidality can coexist with preserved external functioning.
Do not use visible productivity as reassurance against suicide risk. If safety concerns emerge, including self harm thoughts or suicidality, clinical care is crucial. High functioning does not mean harmless.
Why the Distinction Matters Clinically?
Understanding the difference between major depression and high functioning depression has several practical implications.
First, it affects diagnosis. Clinicians must distinguish episodic major depressive disorder from chronic persistent depressive disorder, rule out bipolar disorder, and assess for double depression. The diagnostic process shapes treatment planning, prognosis discussion, and insurance coding.
Second, it affects recognition. If clinicians, families, or patients believe depression must look visibly incapacitating, diagnosis may be delayed. Public health screening recommendations exist partly because many cases are otherwise missed.
Validated screening tools like the PHQ-2 and PHQ-9 can identify depressive symptoms even when they are not externally obvious.
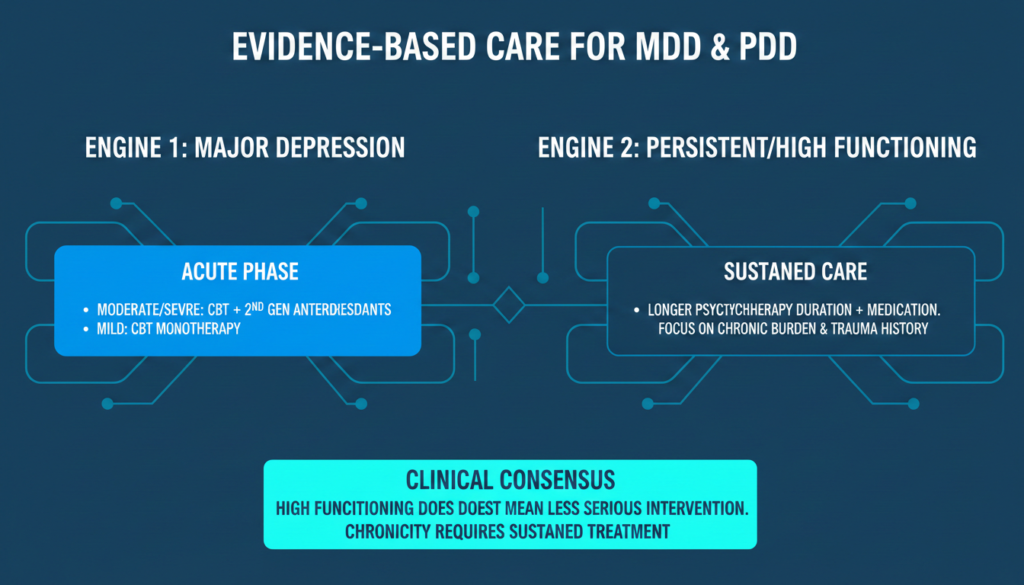
Third, it affects treatment duration and goals. Episodic major depression may respond to acute phase treatment followed by relapse prevention.
Chronic persistent depression requires longer term strategies, attention to cumulative burden, and realistic expectations about recovery timelines.
Fourth, it affects how we talk about functioning. Clinicians should assess functioning across multiple domains, compare with previous baseline, evaluate sustainability of performance, and consider effort cost.
A single question like “Are you still functioning?” is insufficient. True functional assessment includes quality, efficiency, emotional presence, relational engagement, self care, and subjective distress.
Moving Beyond Stereotypes
The most important takeaway is that depression does not always look like obvious collapse. Many people continue to work, parent, socialize, meet deadlines, and appear composed while experiencing ongoing low mood, anhedonia, fatigue, guilt, irritability, low self esteem, concentration problems, sleep disturbance, and hopelessness.
The phrase “high functioning depression” captures this reality but becomes misleading when it implies absence of impairment or lesser need for care.
The more accurate position is that depression exists on a heterogeneous spectrum of presentation, and outward productivity is a poor proxy for severity, risk, or treatment need.
Major depression is more visible. High functioning depression is more concealable. Neither should be trivialized. Both deserve recognition, assessment, and evidence based care.
If you have been pushing through persistent sadness, exhaustion, hopelessness, or emotional numbness while maintaining your responsibilities, you are not imagining it. Your symptoms are real, your distress matters, and help is available.
Depression that is hidden is still depression. Functioning that comes at great internal cost is not the same as wellness.
You don’t have to wait until you can’t get out of bed to reach out. If you’re struggling with symptoms of depression, whether they look like a sudden crash or a years-long weight you’ve been carrying alone, explore Summit Mental Health’s depression treatment designed to meet you where you are and help you move toward genuine recovery.

