Panic attacks can feel like your body is betraying you, heart racing, chest tightening, and a wave of terror that seems to come from nowhere.
Cognitive-behavioral therapy (CBT) reduces panic attacks in roughly half of patients to the point of remission, often within 8 to 12 sessions, by teaching you to face feared sensations rather than avoid them.
This article explains which CBT techniques work best, what to expect during treatment, and how to know if you’re a good candidate for this evidence-based approach.
What is CBT for Panic Disorder?
Cognitive-behavioral therapy for panic disorder is a structured, time-limited treatment that targets the thoughts and behaviors keeping panic attacks alive.
Unlike medication, which manages symptoms while you take it, CBT teaches skills that remain effective long after treatment ends.
The core idea is simple: panic attacks persist because you’ve learned to fear and avoid certain bodily sensations, like a racing heart or shortness of breath.
CBT helps you unlearn that fear by repeatedly exposing you to those sensations in a safe, controlled way. Over time, your brain updates its threat assessment, and the panic response fades.
How CBT Differs from Medication?
When researchers compared CBT to SSRIs and combination treatment in a multicenter trial, they found that medication worked faster in the first few months.
But by six to twelve months after stopping treatment, outcomes were identical across all three groups. CBT’s benefits emerged more slowly but proved more durable once medication was discontinued.
SSRIs come with side effects, sexual dysfunction, weight changes, and withdrawal symptoms when you stop. CBT has no such risks. If you’re looking for a treatment that lasts without ongoing medication, CBT is the stronger choice.
Core CBT Techniques for Panic Attacks
Not all CBT is created equal. Research shows that certain techniques drive most of the improvement, while others add little or even reduce effectiveness.
Interoceptive Exposure: The Most Powerful Tool
Interoceptive exposure means deliberately triggering the physical sensations you fear during a panic attack. You might hyperventilate for 60 seconds, spin in a chair, hold your breath, or run in place until your heart pounds.
The goal is to prove to your brain that these sensations are uncomfortable but not dangerous.
A component analysis of 72 studies found that interoceptive exposure was the single most effective ingredient in CBT for panic disorder. Packages that included it had dramatically higher remission rates than those that didn’t.
One study tested intensive interoceptive exposure against a lower-dose version. The intensive group did the exercises more frequently and at higher intensity early in treatment.
They showed significantly greater reductions in anxiety sensitivity and fear of bodily sensations, and those gains lasted through follow-up. The low-intensity group actually had higher rates of fear sensitization, suggesting that half-measures can backfire.
Common interoceptive exercises include:
- Hyperventilating for 60 to 90 seconds
- Spinning in a chair for 30 to 60 seconds
- Holding your breath for 30 seconds
- Breathing through a straw to simulate shortness of breath
- Running stairs or doing jumping jacks to raise your heart rate
- Brief intense exercise intervals, such as 20-second sprints
Cognitive Restructuring
Cognitive restructuring helps you identify and challenge catastrophic thoughts that fuel panic. If you believe a racing heart means you’re having a heart attack, you’ll panic every time your pulse quickens. CBT teaches you to test those beliefs against evidence.
Your therapist might ask: “How many times has your racing heart actually led to a heart attack?” or “What else could explain this sensation?” Over time, you learn to interpret bodily sensations more accurately, which reduces the fear response.
In Vivo Exposure for Agoraphobia
If panic attacks have led you to avoid certain places, crowded stores, highways, public transit, in vivo exposure helps you reclaim those spaces. You’ll gradually face avoided situations, starting with easier ones and working up to harder challenges.
The key is to stay in the situation long enough for your anxiety to peak and then decline, proving that the feared outcome won’t happen. This process, repeated across different contexts, weakens the avoidance habit and restores your freedom.
What Doesn’t Work as Well?
Some techniques that sound helpful actually show weaker efficacy signals in research. Muscle relaxation and breathing retraining can feel soothing, but they don’t address the core problem: fear of bodily sensations.
In fact, relying on these techniques can become a subtle form of avoidance, reinforcing the idea that certain sensations are dangerous and must be controlled.
Virtual reality exposure has promise for agoraphobia but should be paired with real-world practice to ensure skills generalize beyond the headset.
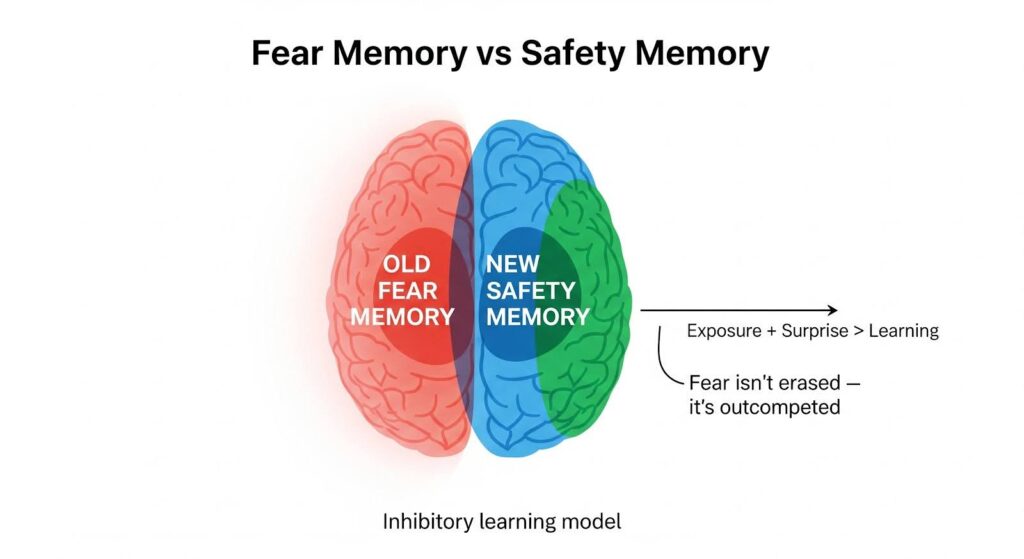
How CBT for Panic Disorder Works: The Inhibitory Learning Model
Traditional exposure therapy aimed to reduce fear through habituation, repeating an exposure until anxiety naturally decreases. But newer research suggests a different mechanism: inhibitory learning.
Exposure doesn’t erase fear memories. Instead, it creates new safety memories that compete with the old fear associations.
The more surprising and varied the exposure, the stronger the safety learning. If you expect a panic attack to spiral into a heart attack and it doesn’t, that prediction error updates your brain’s threat model.
Maximizing Expectancy Violation
To make exposure as effective as possible, therapists now focus on maximizing expectancy violation. Before each exercise, you’ll predict what will happen: “My heart will race, I’ll lose control, and I’ll pass out.” Then you do the exercise and compare the outcome to your prediction. When a catastrophe doesn’t occur, learning is powerful.
Varying the context, intensity, and sequence of exposures strengthens this effect. Doing the same exercise in different locations, at different times of day, and in unpredictable order helps your brain generalize the safety of learning. You’re not just learning that hyperventilating is safe in your therapist’s office, you’re learning it’s safe everywhere.
CBT Treatment Formats: Individual, Group, and Online
One of the most practical findings in recent research is that CBT delivery format doesn’t significantly affect outcomes. Individual therapy, group therapy, and guided self-help all produce similar results.
Individual Therapy
Traditional one-on-one sessions offer the most personalized approach. Your therapist tailors exposures to your specific fears and avoidance patterns. This format works well if you have complex comorbidities or need more intensive support.
Group Therapy
Group CBT is cost-effective and adds a social element. Watching others face their fears can be motivating, and group members often provide valuable support and accountability. Outcomes are equivalent to individual therapy.
Guided Internet-Based CBT
Guided online CBT programs deliver comparable results to face-to-face therapy when they’re disorder-specific and include clinician support. You work through modules at your own pace, with regular check-ins from a therapist via messaging or video.
Unguided self-help, however, doesn’t work as well. The guidance component appears essential for maintaining engagement and ensuring you’re doing exposures correctly.
What to Expect During CBT for Panic Attacks?
A typical CBT course for panic disorder lasts 8 to 12 sessions, though some intensive formats compress treatment into four days or a few weeks.
Sessions 1–2: Psychoeducation and assessment. You’ll learn how panic works, why avoidance maintains it, and how exposure will help. Your therapist will identify your specific triggers and avoidance patterns.
Sessions 3–6: Intensive interoceptive exposure. You’ll do multiple exercises each session, deliberately inducing feared sensations. Your therapist will help you predict outcomes, test those predictions, and process what you learn.
Sessions 7–8: In vivo exposure for agoraphobia. If you’ve been avoiding places or situations, you’ll start facing them in a graded, systematic way.
Sessions 9–10: Cognitive consolidation and relapse prevention. You’ll review what you’ve learned, plan ongoing practice, and develop strategies for handling setbacks.
If you’re taking medication, your therapist may coordinate with your prescriber to taper it gradually as your CBT skills solidify.
CBT vs Medication: Which is Better for Panic Disorder?
The short answer: both work, but CBT lasts longer.
In the SSRI-era trial mentioned earlier, medication and combination treatment reduced symptoms faster in the first nine months.
But after discontinuation, all three groups, CBT alone, SSRI alone, and combination, had identical outcomes at six and twelve months. CBT’s gains emerged more slowly but didn’t fade when treatment ended.
SSRIs are associated with side effects like sexual dysfunction, gastrointestinal upset, and sleep disturbance.
Discontinuation can trigger withdrawal symptoms, dizziness, nausea, anxiety, and sensory disturbances, that are sometimes mistaken for relapse. Gradual tapering reduces this risk but doesn’t eliminate it.
Benzodiazepines reduce panic attack frequency quickly but carry risks of dependence and withdrawal. They may also interfere with exposure learning by blunting the anxiety response you need to experience for CBT to work. Guidelines recommend SSRIs over benzodiazepines as first-line medication for panic disorder.
When to Consider Combination Treatment
If your panic disorder is severe and causing significant functional impairment, starting an SSRI alongside CBT can provide faster relief. The key is to plan for eventual tapering so you can consolidate your CBT skills and maintain gains without medication.
Avoid taking benzodiazepines right before exposure sessions. They can prevent the full anxiety response needed for learning, undermining the therapy’s effectiveness.
Who Benefits Most from CBT for Panic Disorder?
CBT works for most people with panic disorder, but certain profiles predict especially strong outcomes.
High Anxiety Sensitivity
If you’re highly sensitive to bodily sensations and interpret them catastrophically, interoceptive exposure is particularly effective. The more you fear your own heartbeat or breathlessness, the more you stand to gain from learning those sensations are harmless.
Intolerance of Uncertainty
People who struggle with unpredictability benefit from variable exposure strategies. Mixing up the timing, context, and intensity of exposures teaches your brain to tolerate uncertainty, which reduces the need for rigid control.
Preference for Psychological Treatment
If you prefer to avoid medication or have had negative experiences with side effects, CBT is an excellent first-line option. Patients who attribute their improvement to their own efforts rather than a pill tend to maintain gains better over time.
Comorbid Agoraphobia
If panic attacks have led to significant avoidance of places or situations, CBT that includes both interoceptive and in vivo exposure addresses both problems simultaneously. Virtual reality can serve as a stepping stone to real-world exposures when agoraphobia is severe.

Success Rates and Long-Term Outcomes
Roughly 50 to 70 percent of patients achieve remission by the end of CBT treatment, meaning their symptoms drop to minimal or subclinical levels.
Those gains are durable: a long-term follow-up found a relapse rate of only 23 percent over two to fourteen years after exposure-based CBT.
By contrast, relapse rates after stopping SSRIs are higher, and withdrawal symptoms complicate the picture. When researchers followed patients for a year after discontinuing medication, outcomes were no better than those who had received CBT alone.
The takeaway: CBT’s benefits last because you’ve learned a skill, not because you’re taking a pill. Once you know how to face feared sensations without catastrophizing, that knowledge stays with you.
Emerging Innovations in CBT for Panic Attacks
Brief Intermittent Intense Exercise
A recent randomized trial tested brief intermittent intense exercise, short bursts of sprinting or high-intensity intervals, as a form of interoceptive exposure.
Participants who did these exercises showed greater reductions in panic symptoms than those who practiced relaxation, and the benefits lasted through six-month follow-up.
This approach is appealing because it’s easy to self-administer, requires no special equipment, and doubles as a fitness activity.
Acceptance and Commitment Therapy with Interoceptive Exposure
An internet-based ACT program that incorporated interoceptive exposure produced large effect sizes, with 43 percent of participants no longer meeting diagnostic criteria for panic disorder at the end of treatment. Combining acceptance-based strategies with exposure may enhance engagement without diluting the core mechanism.
Practical Tips for Getting the Most from CBT
Start intensive exposure early. Don’t ease into it. Research shows that high-dose interoceptive exposure early in treatment produces better outcomes than gradual approaches.
Vary your practice. Do exposures in different places, at different times, and in unpredictable sequences. This strengthens generalization and reduces the risk of context-specific learning.
Predict and test. Before each exposure, write down what you think will happen. Afterward, compare your prediction to reality. The mismatch is where learning happens.
Avoid safety behaviors. Don’t carry a water bottle “just in case,” sit near exits, or use breathing techniques to control your anxiety during exposures. These subtle avoidances prevent full learning.
Practice between sessions. CBT homework isn’t optional. The more you practice exposures on your own, the faster you’ll improve.
Plan for maintenance. After treatment ends, schedule occasional “booster” exposures to keep your skills sharp. Monthly practice of a few interoceptive exercises can prevent relapse.
When to Seek Professional Help?
If panic attacks are limiting your life, keeping you from work, social activities, or daily routines, it’s time to seek treatment. Panic disorder rarely resolves on its own, and avoidance tends to spread over time.
Look for a therapist trained in evidence-based CBT for panic disorder. Ask specifically about their use of interoceptive exposure and whether they follow an inhibitory learning approach.
Not all therapists who call themselves “CBT therapists” use the techniques that research shows work best.
If you’re already taking medication and want to try CBT, talk to your prescriber about a coordinated plan. Many people successfully taper off medication after building CBT skills, but it should be done gradually and with professional guidance.
Panic attacks don’t have to control your life. CBT offers a clear, evidence-based path to lasting relief by teaching you to face the sensations you fear most.
With the right techniques and consistent practice, you can reclaim the freedom panic has taken from you. If you’re ready to take that step, explore MARR’s anxiety treatment programs to find the support you need.

