You might look productive and put together while feeling empty, exhausted, and joyless inside.
High functioning depression describes a pattern where people meet daily responsibilities but privately struggle with chronic low mood, and it most often overlaps with persistent depressive disorder, a condition affecting about 1.5% of U.S. adults.
This article will help you spot the signs, understand what is really going on, and learn how to treat functional depression effectively.
What is High Functioning Depression, Really?
High functioning depression is not a formal diagnosis. The DSM-5 does not include it, and Medical News Today notes that experts may avoid the phrase because it can be misleading.
Still, the term persists because it captures something real: people who appear successful, organized, and socially engaged while battling persistent sadness, fatigue, and emotional numbness behind closed doors.
In clinical practice, what most people call high functioning depression usually maps onto persistent depressive disorder (PDD), formerly known as dysthymia. PDD involves a depressed mood for most of the day, more days than not, lasting at least two years in adults.
It also includes at least two extra symptoms such as low energy, poor sleep, low self esteem, difficulty concentrating, appetite changes, or hopelessness.
Some people who identify with the term may instead meet criteria for major depressive disorder (MDD), bipolar disorder, anxiety conditions, or partially treated depression.
That is why the label should always lead to a proper clinical evaluation rather than replace one.
Why the “High Functioning” Label Can Be Harmful?
Calling depression “high functioning” can accidentally suggest it is mild or harmless. Everyday Health argues that “high functioning” is not fully functioning and that preserved productivity should never be read as wellness. ColumbiaDoctors compares the experience to a duck: calm on the surface but furiously paddling underneath.
Cleveland Clinic warns that the effort needed to keep performing steadily depletes emotional reserves until burnout hits. The bottom line is that looking okay and being okay are two very different things.
Signs of Functional Depression You Should Not Ignore
One reason functional depression goes unnoticed is that its symptoms blend into daily life. People normalize them as personality traits, stress, or “just the way I am.” Below are the most commonly reported signs across clinical and specialist sources.
Persistent Low Mood or Emotional Flatness
The most basic symptom is a low, dull, or sad mood that hangs around most of the time. Psychology Today describes the main sign of PDD as a low or sad mood most of the day, more days than not, for at least two years.
This may not look like crying or dramatic sorrow. It often shows up as a flattened emotional baseline where nothing feels particularly good or bad.
Fatigue That Sleep Does Not Fix
Low energy is one of the most repeated “hidden” symptoms. You sleep enough hours, but you wake up tired.
Ordinary tasks take far more mental and emotional effort than they appear to from the outside. HelpGuide includes persistent low energy and fatigue as core symptoms of this presentation.
Loss of Joy in Things You Used to Love
Anhedonia, the clinical term for reduced pleasure, is one of the clearest signals that the problem goes beyond ordinary stress. Stress may exhaust you.
Depression strips meaning and pleasure from what should feel rewarding. NIMH lists loss of interest or pleasure in hobbies and activities as a common depressive symptom.
Harsh Self Criticism and Low Self Worth
Low self esteem is formally embedded in PDD descriptions. Many people with functional depression appear driven and successful partly because achievement is being used to compensate for fragile self worth.
Performance is not evidence against depression. Sometimes it is part of the symptom pattern.
Other Common High Functioning Depression Symptoms
| Symptom | How It Often Shows Up |
| Poor concentration or indecision | Compensated through overwork, longer hours, or rigid routines |
| Sleep disturbance | Insomnia or oversleeping, often dismissed as a busy schedule |
| Appetite changes | Undereating or overeating without clear awareness |
| Irritability | Misread as personality, burnout, or “being difficult” |
| Emotional numbness | Success feels strangely unrewarding |
| Social withdrawal after obligations | Performing at work then canceling all plans afterward |
| Perfectionism or constant busyness | Overachievement used as a coping mechanism |
| Physical complaints | Headaches, stomach issues, or chronic aches without clear cause |
| Hopelessness or suicidal thoughts | Can occur even when outward life looks stable |
Why High Functioning Depression Often Goes Unnoticed?
Three forces work together to keep functional depression hidden.
First, preserved productivity masks distress. If someone keeps showing up and delivering results, both others and the person may dismiss symptoms as normal stress. Second, social expectations reward performance, not wellness.
Being busy and reliable is admired, even when it comes at a steep internal cost. Third, people often minimize their own experience. Clarity Clinic notes that the ability to hide symptoms may lead people to “gaslight” themselves into believing they do not need professional help.
This combination means high functioning depression is often hidden not only from others but from the person living with it.
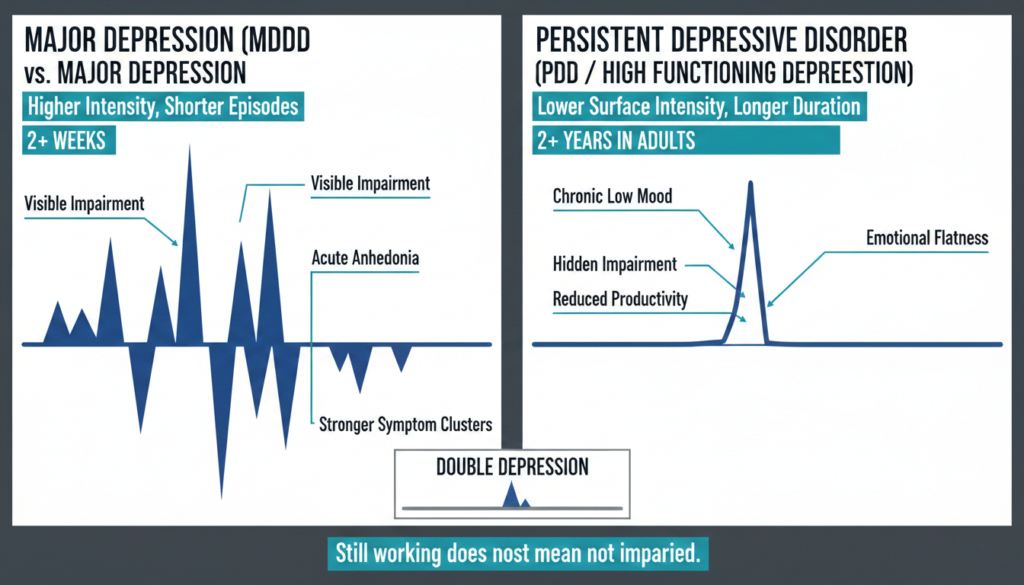
How Functional Depression Differs From Major Depression
Major depressive disorder typically involves more intense symptom clusters over episodes lasting at least two weeks and often causes clearer visible impairment. PDD, by contrast, is less intense on the surface but far more chronic.
WebMD notes that people with dysthymia can also experience periods of major depression, sometimes called double depression, where chronic low grade symptoms suddenly worsen into a severe episode.
A peer reviewed study on work outcomes in dysthymia found that adults with PDD had poorer work performance and productivity than employed controls, even when symptom severity fell in the mild range.
This is important because it directly challenges the idea that “still working” means “not really impaired.”
Risks of Leaving Functional Depression Untreated
Ignoring functional depression does not make it go away. It tends to get worse over time.
Untreated PDD raises the risk of progressing into a full major depressive episode. Chronic emotional masking can lead to burnout when reserves finally run out.
Several sources warn of greater risk for substance misuse, worsening anxiety, physical health problems, and relationship breakdown.
And outward functioning does not protect against suicide risk. NIMH advises contacting 988 or emergency services when thoughts of death or suicide are present.
The most dangerous aspect of the “high functioning” label may be that outsiders underestimate urgency because the person still looks competent.
Treatment Options for High Functioning Depression
Functional depression is treatable. The question is not whether treatment works but which approach fits best based on symptom severity, how long symptoms have lasted, recurrence history, and what has already been tried.
Psychotherapy as a Core Treatment
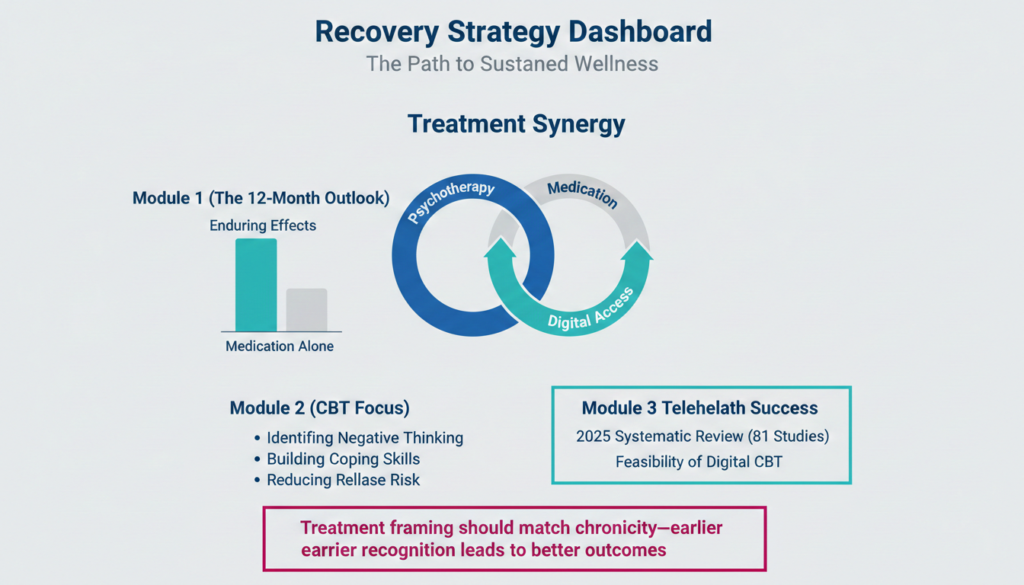
A 2024 systematic review and meta analysis found that psychotherapy and combined treatment had better enduring effects than antidepressant medication alone when measured at least 12 months after treatment ended.
For people with chronic, mild to moderate functional depression, this makes psychotherapy a strong first choice.
Cognitive behavioral therapy (CBT) is the most widely studied approach. It helps identify and change patterns of negative thinking, build coping skills, and reduce relapse risk.
Other effective options include therapies designed specifically for chronic depression and mindfulness based approaches.
Combined Psychotherapy and Medication
When symptoms are moderate to severe, recurrent, or only partially responsive to one approach, combining psychotherapy with antidepressants tends to produce the best results.
The same 2024 review found that combined treatment was significantly better than medication alone over the long term.
Antidepressant Medication
Antidepressants can be helpful, especially when therapy is hard to access or when biological symptoms like severe sleep disruption and appetite loss need faster relief.
However, the evidence suggests medication alone is less durable than psychotherapy or combined care for many patients. It works best as part of a broader plan rather than the entire plan.
Digital and Teletherapy Options
High functioning adults often face barriers like packed schedules, stigma, and long commutes. A 2025 systematic review of 81 studies found that digital and teletherapy CBT formats are feasible, acceptable, and can support sustained improvements in depressive symptoms.
For busy people who might otherwise delay care, flexible digital options can make the difference between getting help and going without.
When Standard Treatment Is Not Enough
If two or more adequate antidepressant trials have failed, the condition may qualify as treatment resistant depression. At that point, options include:
- Repetitive transcranial magnetic stimulation (rTMS) or theta burst stimulation (TBS), which are non invasive brain stimulation methods with good tolerability and growing evidence
- Ketamine or esketamine, which can produce rapid symptom relief within 24 to 72 hours and may reduce acute suicidal thinking
- Electroconvulsive therapy (ECT), which remains one of the most effective options for severe or life threatening depression
- Intensive outpatient programs (IOP) or partial hospitalization programs (PHP), which provide structured daily treatment without full inpatient admission
A 2025 network meta analysis found that ECT, TBS, rTMS, and ketamine were all effective across response and remission outcomes in treatment resistant depression.
Why Getting Assessed Matters More Than the Label?
There is no single “high functioning depression test.” Diagnosis is made through clinical interviews, symptom questionnaires like the PHQ-9, and evaluation of duration, severity, and history.
A proper assessment should look beyond depression alone and consider anxiety, bipolar disorder, substance use, trauma, medical causes of fatigue, and suicide risk.
About 60% of mental health care happens in primary care settings, and 79% of antidepressant prescriptions come from non specialist providers. That means your regular doctor can be a good starting point. The key is not to wait until you “hit bottom.”
If you recognize yourself in the symptoms above, that recognition alone is reason enough to ask for help.
Why Does This Matter?
Functional depression is not a lesser form of depression. It is depression that hides well. The defining feature is not the absence of impairment but the concealment of impairment.
You can be productive, socially present, and outwardly composed while experiencing a chronic condition that quietly erodes your quality of life, your relationships, and your health.
The strongest evidence says psychotherapy centered care, often combined with medication when needed, gives the best chance at lasting recovery. Waiting because you are “still managing” only gives the condition more time to deepen.
If anything in this article felt familiar, you do not have to figure it out alone. Reaching out to a professional is the single most effective step you can take. Explore Summit’s treatment programs that can help you move from just getting by to actually feeling well again.