Feeling persistently down while still managing to show up at work, care for your family, and meet your responsibilities can leave you wondering if what you’re experiencing is “real” depression or just stress.
Unipolar depression is a mood disorder characterized by depressive episodes without the manic or hypomanic phases seen in bipolar disorder, affecting roughly 2.5% of adults over their lifetime and often going unrecognized for years when symptoms are chronic and low-grade.
This article explains what unipolar depression is, how it differs from bipolar depression, the symptoms and causes clinicians look for, and the evidence-based treatments that can help you reclaim your well-being.
Understanding Unipolar Depression
Unipolar depression refers to depressive disorders that involve only depressive symptoms, without the elevated mood states that define bipolar disorder.
The term encompasses major depressive disorder (MDD), which features distinct episodes of severe depression, and persistent depressive disorder (PDD), formerly called dysthymia, which involves chronic low-grade depression lasting at least two years in adults.
When someone experiences a major depressive episode during the course of persistent depressive disorder, clinicians now diagnose both conditions simultaneously.
This dual coding approach, clarified in DSM-5-TR guidance, helps capture the full picture: a chronic baseline of dysphoria punctuated by more severe episodes. This pattern, sometimes called “double depression,” is common but frequently overlooked because the persistent symptoms become normalized as “just how I am.”
The distinction between unipolar and bipolar depression matters enormously for treatment. Antidepressants are a mainstay for unipolar depression, but in bipolar depression they can trigger mood switching or destabilization when used without mood stabilizers.
Misdiagnosis in either direction carries risks: treating undiagnosed bipolar depression as unipolar can lead to antidepressant-associated mood switching, while mislabeling unipolar depression as bipolar can result in unnecessary exposure to antipsychotics or mood stabilizers with significant side effects.
Unipolar Depression Symptoms
Symptoms of unipolar depression fall into emotional, cognitive, physical, and behavioral domains.
For a diagnosis of major depressive disorder, you must experience at least five symptoms nearly every day for at least two weeks, including either depressed mood or loss of interest or pleasure.
Core Emotional and Cognitive Symptoms
- Persistent sad, empty, or hopeless mood
- Loss of interest or pleasure in activities once enjoyed
- Feelings of worthlessness or excessive guilt
- Difficulty concentrating, making decisions, or remembering
- Recurrent thoughts of death or suicide
Physical and Behavioral Symptoms
- Significant weight loss or gain, or changes in appetite
- Insomnia or sleeping too much
- Psychomotor agitation or slowing noticeable to others
- Fatigue or loss of energy nearly every day
- Withdrawal from social activities and relationships
In persistent depressive disorder, symptoms are present more days than not for at least two years but may not always meet the full threshold for a major depressive episode.
This chronicity often leads people to dismiss their suffering as personality or “just stress,” delaying recognition and treatment for years.
High-functioning individuals may continue to meet work and family obligations while experiencing significant internal distress.
This outward competence can mask the severity of the condition, making it easy for both the person and their clinician to underestimate the burden.
Unipolar Depression vs Bipolar Depression
The difference between unipolar and bipolar depression lies in the presence or absence of manic or hypomanic episodes.
Unipolar depression involves only depressive states, while bipolar disorder includes periods of elevated, expansive, or irritable mood with increased energy.
Key Distinguishing Features
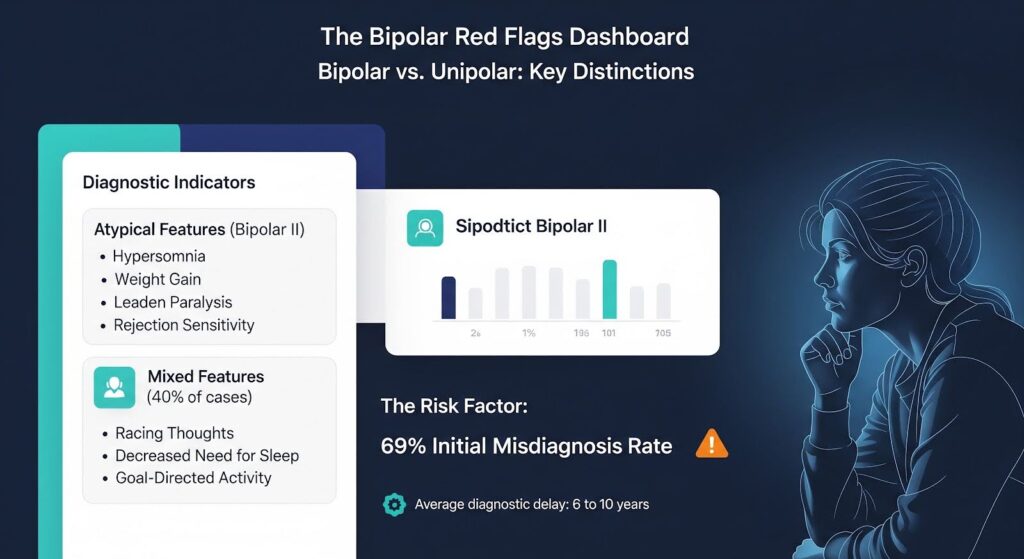
Bipolar depression often presents with atypical features such as hypersomnia, increased appetite or weight gain, leaden paralysis (heavy feeling in limbs), and interpersonal rejection sensitivity. Research shows these features have moderate specificity for bipolar II disorder but low sensitivity, meaning they help confirm bipolarity when present but miss many cases when absent.
Mixed features during depression, such as racing thoughts, decreased need for sleep, or increased goal-directed activity, are more common in bipolar depression. DSM-5 introduced a mixed features specifier to capture these subsyndromal manic symptoms, which occur in up to 40% of depressive episodes in bipolar disorder and signal higher risk for mood switching and suicidality.
Diagnostic delay in bipolar disorder averages six to ten years, with 69% of patients initially misdiagnosed, often as unipolar depression. This delay contributes to inappropriate antidepressant monotherapy, increased hospitalizations, and worse long-term outcomes.
Screening Tools and Their Limitations
Clinicians use tools like the Mood Disorder Questionnaire (MDQ) and Hypomania Checklist-32 (HCL-32) to screen for bipolar disorder.
The HCL-32 shows higher sensitivity for bipolar II (0.90 versus 0.83 for MDQ), while the MDQ offers better specificity. However, both tools are influenced by comorbid conditions, which can inflate scores regardless of true bipolar status.
Importantly, these bipolar screens do not detect unipolar depression. A negative screen provides no information about chronic depressive burden, and overreliance on bipolar detection tools can leave persistent unipolar depression invisible in clinical workflows.
| Feature | Unipolar Depression | Bipolar Depression |
|---|---|---|
| Mood episodes | Depressive only | Depressive plus manic/hypomanic |
| Atypical features | Present in some cases | More common; moderate specificity |
| Mixed features | Typically absent | Common (up to 40% of episodes) |
| Antidepressant response | Generally safe as monotherapy | Risk of mood switching without stabilizers |
| Screening tools | PHQ-9, chronicity assessment | MDQ, HCL-32 for bipolar risk |
Causes and Risk Factors
Unipolar depression arises from a complex interplay of biological, psychological, and environmental factors. No single cause explains all cases, but several well-established risk factors increase vulnerability.
Biological Factors
Genetics play a significant role. Having a first-degree relative with depression roughly doubles your risk. Neurotransmitter systems involving serotonin, norepinephrine, and dopamine are implicated, though the mechanisms are more complex than simple “chemical imbalance” models suggest.
Chronic medical conditions, hormonal changes, and certain medications can trigger or worsen depression. Inflammation and stress-response system dysregulation are increasingly recognized as contributing pathways.
Psychological and Social Factors
Early life adversity, trauma, and chronic stress shape depression risk. Cognitive patterns such as rumination, negative self-talk, and learned helplessness maintain depressive states. Interpersonal difficulties, social isolation, and lack of supportive relationships amplify vulnerability.
For high-functioning professionals, structural and cultural factors add unique pressures. Fear of career consequences from disclosing mental health conditions has historically deterred help-seeking.
Although major reforms to licensure and credentialing applications now focus on current impairment rather than past diagnosis or treatment, residual stigma and self-normalization of chronic symptoms continue to delay recognition.
Why High-Functioning Unipolar Depression Goes Undetected?
Chronic, low-grade depression in high-functioning individuals often remains hidden for years. Three factors converge to create this blind spot.
First, persistent depressive disorder is ego-syntonic. When you’ve felt down more days than not for years, it becomes part of your identity rather than a treatable condition. You rationalize the distress as personality, stress, or “just burnout.”
Second, clinical training and screening workflows emphasize bipolar detection and episode severity. When bipolar red flags are absent and you’re still meeting responsibilities, clinicians may underestimate the burden or default to non-psychiatric explanations.
Third, structural disincentives have historically suppressed disclosure. Intrusive mental health questions on licensing and credentialing forms created fear of career repercussions. Surveys indicate roughly 40% of physicians report reluctance to seek care due to these concerns, with reluctance approximately 20% higher in states with broad mental health inquiries.
Reforms are accelerating. As of January 2026, more than 2,100 facilities covering over 438,000 credentialed health workers have adopted impairment-only questions aligned with recommendations from the American Medical Association, Federation of State Medical Boards, and National Association Medical Staff Services. These changes reduce barriers, but awareness and implementation remain uneven.
Treatment Options for Unipolar Depression
Effective treatment for unipolar depression typically combines psychotherapy, medication, and lifestyle interventions. The specific approach depends on severity, chronicity, and individual preferences.
Psychotherapy
Cognitive Behavioral Therapy (CBT) is one of the most extensively studied treatments for depression. It helps you identify and change negative thought patterns and behaviors that maintain depressive states.
Dialectical Behavior Therapy (DBT) adds skills for emotion regulation, distress tolerance, and interpersonal effectiveness, particularly useful when depression coexists with trauma or emotional dysregulation.
Interpersonal therapy focuses on relationship patterns and life transitions that contribute to depression. For trauma-related depression, Eye Movement Desensitization and Reprocessing (EMDR) can reduce the emotional charge of traumatic memories.
Medication
Antidepressants are a cornerstone of pharmacologic treatment for unipolar depression. Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) are typically first-line options due to their efficacy and tolerability.
Before starting antidepressants, clinicians should screen for bipolar risk. In adults initially diagnosed with unipolar depression, prior antidepressant exposure is associated with higher subsequent incidence of mania or bipolar disorder, with adjusted hazard ratios significant for SSRIs and venlafaxine. This association underscores the importance of careful assessment rather than contraindication.
When mixed features are present during a depressive episode, antidepressant monotherapy should be avoided. Mood stabilizers or atypical antipsychotics may be added or used as primary agents to reduce the risk of activation or switching.
Holistic and Lifestyle Interventions
Exercise, sleep hygiene, nutrition, and stress management support recovery and reduce relapse risk. Mindfulness practices, yoga, and meditation can improve emotional regulation and reduce rumination. Social connection and meaningful activity counter isolation and anhedonia.
Dual Diagnosis and Co-Occurring Conditions
When depression coexists with substance use disorders, anxiety, PTSD, or other mental health conditions, integrated treatment addressing all conditions simultaneously produces better outcomes than sequential or siloed approaches.
When to Seek Professional Help?
You should seek professional evaluation if depressive symptoms persist for more than two weeks, interfere with work or relationships, or include thoughts of self-harm or suicide. Even if symptoms are chronic and you’ve “managed” for years, treatment can significantly improve quality of life and functioning.
If you’ve been treated for depression but continue to experience activation, irritability, or mood swings on antidepressants, discuss bipolar screening with your clinician. Conversely, if you’ve been labeled with bipolar disorder but lack clear manic or hypomanic episodes, a second opinion may clarify your diagnosis and optimize treatment.
For professionals concerned about licensure or credentialing consequences, know that impairment-only inquiries are now standard in many jurisdictions. Seeking care when you are not impaired does not require disclosure and supports long-term career sustainability.
Moving Forward with Confidence
Unipolar depression, whether episodic or persistent, is a treatable condition with strong evidence for psychotherapy, medication, and integrated care.
Recognizing chronic depressive symptoms as a legitimate illness rather than a character flaw or inevitable stress response is the first step toward recovery. Accurate diagnosis distinguishes unipolar from bipolar depression and guides safer, more effective treatment choices.
If you’ve been living with persistent low mood, loss of interest, or functional impairment for months or years, you don’t have to continue suffering in silence. Compassionate, evidence-based care can help you reclaim energy, connection, and purpose.
Ready to take the next step? Reach out to explore outpatient mental health treatment customized to your needs and schedule.

