Depression can feel like being trapped in a cycle of overwhelming emotions, self-criticism, and withdrawal.
If you’ve tried standard treatments without lasting relief, especially when your depression comes with intense mood swings, relationship struggles, or thoughts of self-harm, Dialectical Behavior Therapy offers a different path.
DBT teaches concrete skills to survive emotional storms, regulate your responses, and build a life worth living even when depression makes everything feel impossible.
This article explains how DBT works for depression, which techniques matter most, and when this approach makes the most sense for your recovery.
What DBT is and Why It Matters for Depression?
Dialectical Behavior Therapy was originally developed by Marsha Linehan in the late 1980s for chronically suicidal individuals with borderline personality disorder who found standard cognitive behavioral therapy too invalidating or critical.
Over time, DBT evolved into a broader, evidence-based psychotherapy used across multiple clinical populations characterized by emotion dysregulation, self-harm, suicidality, and complex comorbidity.
DBT is not the default first-line psychotherapy for depression in the way that CBT or behavioral activation often are. However, it has become increasingly relevant for patients whose depression is recurrent, emotionally dysregulated, suicidal, treatment-resistant, or complicated by anxiety, trauma, personality pathology, interpersonal instability, or poor coping under stress.
The distinctive therapeutic model combines acceptance-based strategies such as mindfulness and validation with change-oriented behavioral methods. This produces a structured treatment system centered on mindfulness, emotion regulation, distress tolerance, and interpersonal effectiveness.
How DBT Differs From Other Depression Treatments?
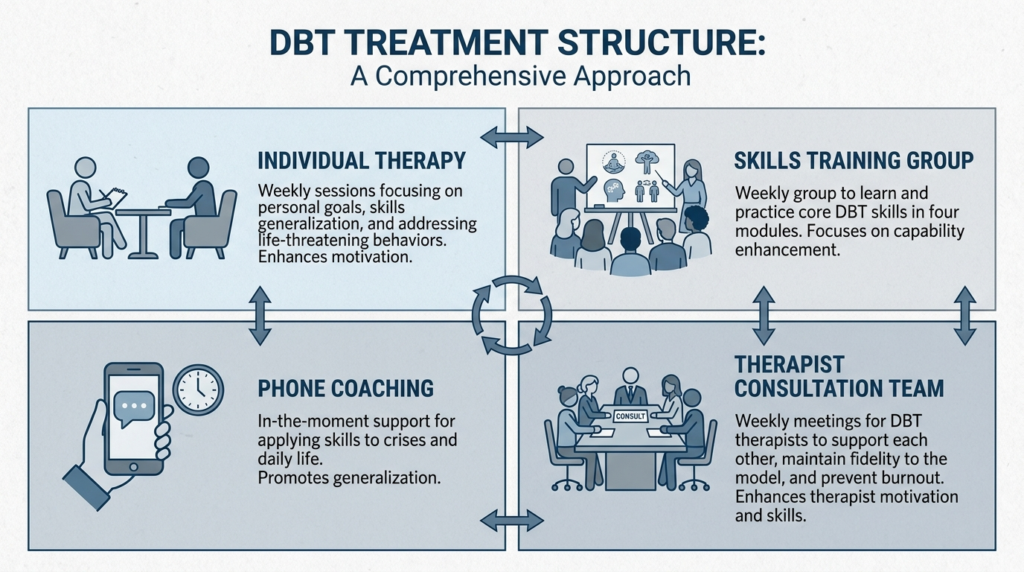
Standard DBT is more than a simple coping-skills class. Comprehensive DBT typically includes weekly individual therapy, weekly skills training group, between-session phone coaching, and a therapist consultation team. This multicomponent structure distinguishes it from other approaches.
The defining dialectical principle is the balancing of acceptance and change. Patients are taught that two apparently opposite truths can coexist: they are doing the best they can, and they need to try harder or differently. They must accept current reality, and they must also work to change harmful patterns.
For depression, this stance is especially relevant. Depressive states frequently involve self-condemnation, rigid all-or-nothing thinking, hopelessness about change, paralysis in the face of painful emotion, and chronic invalidation of one’s own internal experience. DBT responds by simultaneously validating suffering and training concrete behavioral responses.
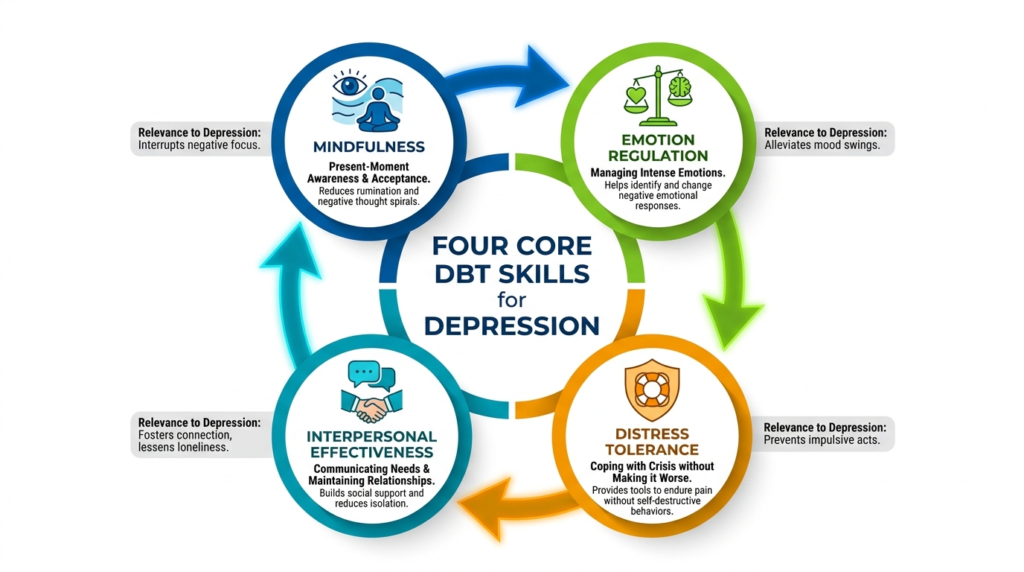
The Four Core DBT Skills for Depression
DBT organizes skills into four core modules that map directly onto common depressive maintaining processes.
Mindfulness
Mindfulness increases awareness without fusion or judgment. It addresses rumination, self-criticism, and automatic negative spirals.
You learn to notice “I am having the thought that I’m a failure” rather than simply accepting it as truth. This skill restores contact with immediate experience, which can counter depressive narrowing and disengagement.
Emotion Regulation
Emotion regulation improves identification and modulation of emotional states. It counteracts persistent sadness, irritability, shutdown, and reactivity. Two particularly useful techniques are Check the Facts and opposite action.
Check the Facts involves evaluating whether an emotional reaction matches the actual facts of the situation, especially when emotions are driven by interpretations or assumptions rather than directly observable events.
Depression often involves overgeneralization and certainty about negative meaning. Check the Facts helps slow that interpretive cascade.
Opposite action helps you recognize an emotion-driven behavior and choose an alternative. If shame or sadness says “hide, lie in bed, cancel, do nothing,” opposite action may mean shower, text a friend, go outside, complete one task, or attend the appointment.
Distress Tolerance
Distress tolerance builds non-destructive coping during crises. It addresses suicidal urges, self-harm risk, panic, and overwhelming hopelessness. These skills are designed for situations where the immediate goal is not to solve the problem or change the emotion, but to avoid making things worse.
Practical strategies include grounding, deep breathing, self-soothing, distraction, and radical acceptance. For depressed patients, these skills can create enough stability to prevent self-destructive behavior, catastrophic texting, quitting responsibilities impulsively, or collapsing into numbing habits.
Interpersonal Effectiveness
Interpersonal effectiveness improves communication and relationship functioning. It reduces isolation, conflict, rejection sensitivity, and unmet needs. Depression is strongly maintained by social processes such as withdrawal, conflict, chronic invalidation, low assertiveness, fear of rejection, and unstable relationships.
DBT’s interpersonal effectiveness module provides explicit training in asking for needs, setting limits, validating others, and maintaining self-respect in relationships. This may be especially useful in depression with strong relational triggers.
Evidence for DBT in Depression
Current evidence for DBT in depression is promising but uneven. A CADTH evidence review found mixed results on depressive symptoms overall, with several randomized controlled trials showing no significant endpoint advantage over active comparators.
However, at least one pilot RCT found markedly better short-term depressive outcomes for DBT-based psychoeducation versus wait-list.
Emerging work suggests DBT may speed improvement in anxiety and emotion dysregulation even when endpoint differences are modest.
In a pilot RCT of DBT skills for transdiagnostic emotion dysregulation, both DBT and an activity-based support group improved emotion dysregulation, but DBT participants improved significantly faster, with a very large effect size, even though follow-up endpoint differences were not significant.
This is an important nuance. A therapy can be clinically valuable not only if final outcomes are superior, but also if it improves patients more quickly, reduces crises earlier, and accelerates acquisition of adaptive coping. For depressed patients at high risk, speed of stabilization can matter greatly.
DBT Skills Use as a Mechanism of Change
One of the most practically important findings is that using the skills appears to matter, not merely learning about them.
One study found that DBT skills use fully mediated improvements in depression over time. The same paper argues that DBT conceptualizes lack of behavioral activation as a skills deficit and teaches behavioral activation principles within the emotion regulation module.
This creates an important bridge between DBT and behavioral activation research. Behavioral activation has robust evidence for depression and works partly by increasing activity and reinforcement.
DBT may achieve part of its antidepressant effect through overlapping activation-based mechanisms, but embeds them inside a broader emotion-regulation and crisis-management framework.
When DBT Makes the Most Sense for Depression?
DBT is best understood not as a universal replacement for established depression therapies, but as a highly relevant, mechanism-rich, and clinically plausible intervention for depressive presentations marked by emotional dysregulation, suicidality, chronicity, or treatment resistance.
The strongest present justification for DBT in depression is selective rather than universal. It is most compelling as an augmentation or adaptation strategy for complex depression.
Depression With Severe Emotion Dysregulation
Patients whose mood problems are inseparable from affective volatility, impulsivity, shame spirals, intense anger, or difficulty recovering from stress are strong candidates for DBT.
Depression With Suicidality or Self-Harm Risk
DBT’s broader evidence base is strongest in suicidal populations, making it especially suitable when depressive episodes involve recurrent crisis behavior.
Treatment-Resistant Depression With Complex Psychosocial Features
For treatment-resistant depression, the evidence base remains underdeveloped. A 2024 publication on DBT augmentation for TRD is a protocol for a first comprehensive systematic review and meta-analysis rather than a completed synthesis.
However, DBT is especially relevant when repeated medication trials have not resolved the coping, interpersonal, and emotion-regulation patterns sustaining depression.
Contemporary protocols estimate that about 30% of patients with MDD experience treatment-resistant depression, highlighting the need for effective augmentation strategies beyond medication alone.
DBT has become one of the therapies considered in this context because it directly targets emotion dysregulation, maladaptive coping, and behavioral patterns that often sustain depressive suffering.
Depression With Co-Occurring Anxiety
Several trials found that DBT participants improved significantly faster in anxiety severity. DBT may speed anxiety improvement and reduce emotional overwhelm, which can indirectly support depression recovery even if pure depressive endpoint scores do not always separate strongly from comparator treatments.
Practical DBT Techniques You Can Use
While comprehensive DBT requires professional guidance, several techniques can be practiced independently to support depression recovery.
Mindful Breathing and Grounding
When you notice yourself spiraling into rumination or self-attack, pause and focus on your breath for one minute. Notice the sensation of air moving in and out. This simple practice helps distinguish feelings from facts and thoughts from events.
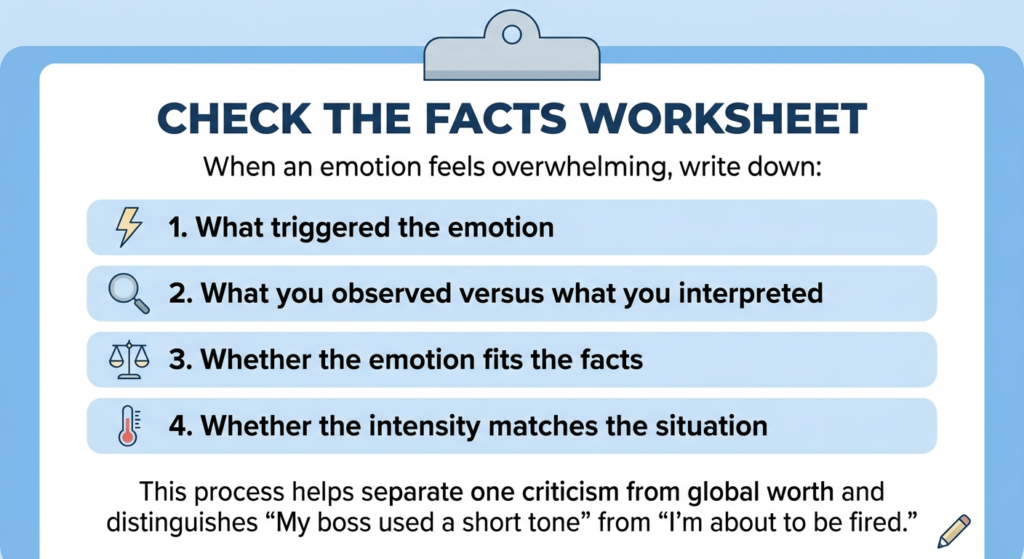
Check the Facts Worksheet
When an emotion feels overwhelming, write down:
- What triggered the emotion
- What you observed versus what you interpreted
- Whether the emotion fits the facts
- Whether the intensity matches the situation
This process helps separate one criticism from global worth and distinguishes “My boss used a short tone” from “I’m about to be fired.”
Opposite Action Practice
Identify one behavior depression is pushing you toward today. Then do the opposite:
- If depression says stay in bed, get up and shower
- If it says cancel plans, attend for 15 minutes
- If it says you’re worthless, text one friend
- If it says hide your needs, make one clear request
Distress Tolerance for Crisis Moments
When hopelessness spikes or you feel overwhelmed:
- Place your hands in cold water
- Name five things you can see
- Practice paced breathing: inhale for four counts, exhale for six
- Use self-soothing: listen to calming music, wrap in a soft blanket
DBT Delivery Formats and Accessibility
Standard comprehensive DBT programs generally include weekly individual therapy, weekly skills group, between-session phone coaching, and weekly therapist consultation team. Typical outpatient structure is around three hours per week, and many programs run for six months to one year.
Not all depression-oriented DBT uses the full standard model. Adapted forms include 12-week DBT-based psychoeducation, 10-week emotion regulation plus mindfulness groups, 15-week modified DBT-informed individual psychotherapy for depressive and anxiety disorders, and DBT-informed partial hospital or intensive outpatient programs.
Telehealth DBT has become increasingly viable. Studies indicate widespread adoption among clinicians, with cautious optimism regarding telehealth DBT. The core DBT functions can be preserved online if the program maintains individual therapy, skills training, coaching pathways, and consultation support.
Digital formats are best viewed as amplifiers of skill use, not replacements for full treatment in high-risk or complex cases. For depression and anxiety, they are likely most useful when they prompt practice during predictable risk windows, store diary cards and skill reminders, coach the next step during emotional escalation, and integrate with therapist guidance.
What to Expect in DBT Treatment?
Some DBT programs require a pretreatment phase lasting around four to six weeks to orient patients, assess commitment, and begin diary card use. This structured entry process may be especially useful for depressed patients with hopelessness, ambivalence, inconsistent attendance, or prior dropout from treatment.
The components serve different functions. Individual therapy provides case formulation, hierarchy of targets, chain analysis of depressive crises, and personalized application of skills. Skills group offers repeated practice in mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness.
Phone coaching provides real-time help using skills before a crisis escalates. The consultation team supports therapist adherence and effectiveness in complex or high-risk cases.
This is one reason DBT can be particularly suitable for depressed patients who struggle not with insight alone, but with generalizing skills into moments of acute distress.
Limitations and Realistic Expectations
The strongest supplied evidence does not support a blanket claim that DBT is universally superior for depressive disorders. Evidence is mixed, and many studies are small or adapted.
For straightforward, uncomplicated depression without major dysregulation or crisis risk, simpler and more directly validated treatments such as behavioral activation or CBT may often be more efficient first choices.
DBT is not merely a list of coping skills. Mindfulness is one module. DBT’s depression relevance depends equally, and often more, on emotion regulation, distress tolerance, interpersonal effectiveness, and the full treatment structure.
Skills group can be valuable, but standard DBT includes four modes. Research findings from skills-only studies should not be generalized automatically to comprehensive DBT, and vice versa.
Moving Forward With DBT for Depression
DBT helps depression by teaching patients how to experience painful emotion without collapse, regulate behavior under stress, rebuild relationships, and move from chronic invalidation and helplessness toward skillful action. For the right depressive presentations, that is not a peripheral advantage but the central therapeutic need.
The most defensible position from current evidence is that DBT for depression is best understood not as a universal replacement for established depression therapies, but as a highly relevant, mechanism-rich, and clinically plausible intervention for depressive presentations marked by emotional dysregulation, suicidality, chronicity, or treatment resistance.
If your depression involves intense emotional reactivity, relationship chaos, self-harm urges, or repeated treatment failures, DBT may offer the structured support and practical tools you need to build stability and move toward recovery. Reach out to The Summit Wellness Group to learn whether DBT-informed treatment is right for you.

