Many people struggle with difficult thoughts and feelings that seem to control their lives. Acceptance and Commitment Therapy (ACT) helps you build psychological flexibility, the ability to stay present with discomfort while taking action toward what truly matters to you.
Recent research shows ACT significantly improves depression, anxiety, and functioning across diverse populations, often by changing how you relate to inner experiences rather than eliminating them.
This article explains what ACT is, how it works, and what conditions it treats most effectively.
Understanding ACT: A Process-Based Behavioral Therapy
Acceptance and Commitment Therapy is a modern behavioral psychotherapy that emerged from the cognitive-behavioral tradition but developed a distinct identity through its grounding in functional contextualism and Relational Frame Theory.
Rather than focusing primarily on eliminating unwanted thoughts and feelings, ACT seeks to increase psychological flexibility: the capacity to remain open to internal experience, stay in contact with the present moment, and behave in ways that serve personally chosen values even when discomfort is present.
This orientation differentiates ACT from models centered mainly on cognitive content change or symptom suppression. The therapy was developed in the 1980s by Steven C. Hayes, Kelly Wilson, and Kirk Strosahl as part of a broader scientific strategy called contextual behavioral science.
In that framework, therapy is not merely a collection of techniques but an applied extension of a broader model of human behavior, language, and learning.
ACT is often described as a “third wave” cognitive-behavioral therapy, but this description is incomplete. The model did not arise outside behavioral science; it emerged from within the CBT and behavioral therapy tradition and was developed as part of a coherent scientific approach linking theory, measurement, and intervention.
The Core Aim: Building Psychological Flexibility
The most concise and accurate description of ACT is that it aims to build psychological flexibility. Across authoritative ACT sources, psychological flexibility is defined as the ability to contact the present moment more fully and to persist in or change behavior when doing so serves chosen values.
This means ACT does not ask whether people can get rid of pain, fear, sadness, self-doubt, or traumatic memories first. It asks whether they can learn to relate differently to these experiences so that life does not become organized around avoiding them.
This emphasis matters because many common psychological struggles are intensified by experiential avoidance—attempts to suppress, escape, control, or outmaneuver unwanted inner experiences.
ACT explicitly frames acceptance as the opposite of experiential avoidance. In ACT, “acceptance” does not mean liking pain, resigning oneself to injustice, or refusing change. It means a willingness to make space for difficult thoughts, feelings, sensations, and urges when struggling with them is itself making life narrower, less workable, or less aligned with values.
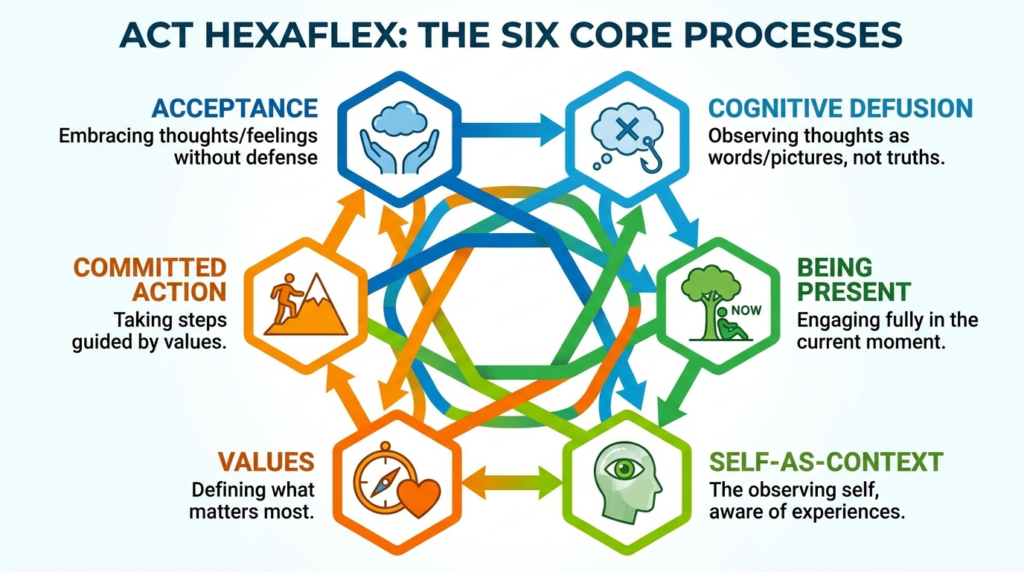
The Six Core Processes of ACT
ACT operationalizes psychological flexibility through six interrelated processes: acceptance, cognitive defusion, being present, self-as-context, values, and committed action.
These are often depicted as a hexaflex, but they are not meant to be rigid compartments. They are overlapping pathways that together reduce rigidity and increase flexible, values-guided behavior.
Acceptance
Acceptance in ACT is defined as the opposite of experiential avoidance. It is a willingness to experience difficult internal events rather than trying to suppress, escape, or control them. This does not mean passively enduring abuse, injustice, or danger. Rather, it targets the internal struggle that often amplifies suffering.
For example, a person with panic symptoms may spend years trying to prevent any sign of bodily arousal. ACT would help them notice that the fight against anxiety may be constricting life more than anxiety itself. Acceptance makes room for fear so that valued action, travel, intimacy, work, parenting, can resume.
Cognitive Defusion
Defusion involves observing thoughts mindfully rather than avoiding or disputing them. If cognitive fusion means becoming entangled with thoughts as literal truths or commands, defusion means relating to them with more distance and flexibility.
For instance, instead of being fused with “I’ll embarrass myself, so I can’t go,” you might notice “I’m having the thought that I’ll embarrass myself.” That linguistic shift may seem modest, but it changes the function of the thought. The thought becomes an event in awareness, not an unquestioned controller of action.
Being Present
Present-moment awareness involves contacting ongoing experience with openness and flexibility. It is not simply relaxation.
It helps people notice what is happening now rather than operating entirely from automatic worry, rumination, or self-judgment. Being present allows more accurate contact with environmental contingencies and with one’s own needs and opportunities.
Self-as-Context
Self-as-context is one of ACT’s more abstract but clinically important processes. It refers to a stable perspective from which thoughts, feelings, roles, and identities can be observed without being equated with the whole self.
This is useful for people whose suffering is intensified by rigid identity stories such as “I am broken,” “I am weak,” or “I am my diagnosis.”
Values
Values are not goals in the narrow sense. They are chosen qualities of action, directions one wants to embody, such as compassion, honesty, courage, curiosity, or loyalty.
ACT gives values a central role because they provide a reason to tolerate discomfort. Without values, acceptance can feel like pointless suffering. With values, willingness becomes meaningful.
Committed Action
Committed action refers to practical behavior change guided by values. It often includes goal-setting, persistence, skills use, and behavioral activation. ACT is not only reflective or experiential; it is also action-oriented. Psychological flexibility ultimately shows up in what a person does.
What Conditions Does ACT Treat?
ACT is best understood as a broad-spectrum, process-based therapy rather than a niche intervention for one disorder. The strongest direct evidence concerns depression, anxiety, stress, and psychological distress, with evidence also extending to health anxiety, workplace well-being, chronic pain, and trauma-related conditions.
Depression
The clearest evidence supports ACT for depression. A 2025 meta-analysis of 13 randomized controlled trials involving 1,362 adults with depression found that ACT significantly improved depression with a standardized mean difference of -0.66, anxiety with SMD of -0.43, and psychological flexibility with SMD of 0.50. These effects were maintained at follow-up, suggesting medium-term durability.
A related 2025 systematic review and meta-analysis of 10 randomized controlled trials also found significant improvements in diagnosed depression, with SMD of -0.69 for depression, -0.64 for anxiety, and 0.35 for psychological flexibility.
Subgroup findings suggested that group ACT may be more effective than individual ACT for people with depression.
Anxiety
ACT is also used for anxiety-related problems. The depression-focused meta-analyses found accompanying reductions in anxiety symptoms, which is consistent with ACT’s transdiagnostic orientation. Internet ACT research further supports small but reliable improvements in anxiety outcomes across diverse conditions.
ACT is conceptually well suited to anxiety because anxiety disorders often involve fear of internal experiences themselves: bodily arousal, intrusive thoughts, uncertainty, embarrassment, or memories. ACT directly targets the struggle with those experiences rather than solely the content of anxious predictions.
Chronic Pain
Chronic pain is one of the most extensively supported ACT applications. A 2023 systematic review and meta-analysis of 21 trials with 1,962 participants found effects favoring ACT on pain acceptance, quality of life, pain-related functioning, pain intensity, anxiety, and depression.
This evidence strongly suggests that ACT techniques are especially effective for changing pain-related functioning, increasing acceptance, reducing emotional distress linked to pain, and improving life engagement despite symptoms.
Chronic pain is a domain where relentless attempts to eradicate discomfort can easily become part of the disability cycle. ACT’s acceptance techniques do not deny pain; they directly address the secondary suffering created by struggle, avoidance, and life constriction.
Trauma and PTSD
The supplied evidence suggests growing support for ACT in trauma-related problems. In military personnel, comprehensive reviews report that ACT has shown significant effectiveness in alleviating PTSD symptoms, though its superiority over other therapies remains uncertain and more randomized comparisons are needed.
ACT may be especially useful in trauma when experiential avoidance is severe, interpersonal functioning is eroded, clients are unwilling or unable to engage in traditional trauma-focused exposure immediately, or comorbidity complicates single-disorder protocols.
Traumatic Brain Injury
A 2025 systematic review and meta-analysis of ACT for adults with TBI found that across four randomized controlled trials with 227 participants, ACT significantly improved combined depression and anxiety, psychological flexibility, mental health-related quality of life, and functional disability.
However, ACT did not significantly improve rehabilitation participation or physical health-related quality of life.
This pattern is theoretically coherent. ACT is built to change the relationship to internal experience and enhance values-based action; it is not primarily a neurocognitive retraining protocol or a physical rehabilitation method.
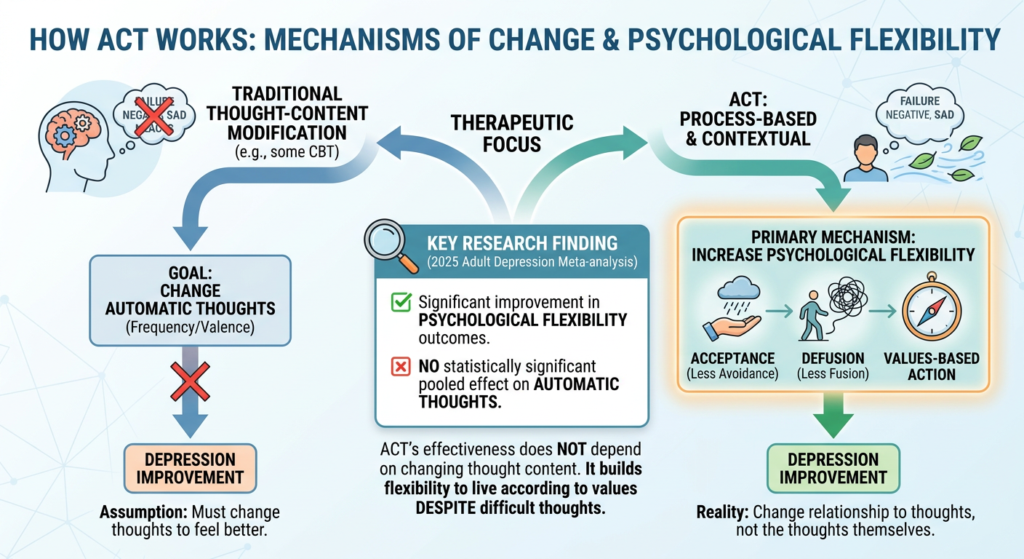
How ACT Works: Mechanisms of Change
The strongest mechanism claim supported by research is that ACT works primarily through increasing psychological flexibility. That conclusion is supported by ACT’s foundational model, repeated definitions across professional sources, and meta-analytic findings showing improvements in flexibility outcomes.
Importantly, the 2025 adult depression meta-analysis found no statistically significant pooled effect on automatic thoughts.
This is one of the most theoretically meaningful findings in the evidence base. ACT’s depression effects appear genuine, but they do not seem to depend primarily on changing the frequency or valence of automatic thoughts. Instead, the more likely pathway is increased flexibility, less fusion, less experiential avoidance, and greater values-based action despite depressive cognition.
This gives ACT a meaningful distinctiveness relative to therapies whose central mechanism is assumed to be thought-content modification. That does not prove ACT is superior to CBT overall. It does show that ACT is not merely CBT with different branding.
Common ACT Techniques and Exercises
Because ACT is a process-based therapy, techniques are chosen through functional assessment rather than therapist preference. The most important “techniques” are not isolated exercises, but functional methods for changing how people relate to internal experience while increasing effective action.
Mindfulness and Present-Moment Exercises
These techniques target awareness and attentional flexibility. Examples include breath tracking for one to three minutes, sensory grounding, mindful eating or walking, and noticing thoughts, feelings, and urges as current events. The purpose is to interrupt autopilot, rumination, and threat-based scanning.
Acceptance and Willingness Exercises
These target experiential openness. Examples include asking “Can you allow this sensation to be here for the next 10 seconds?” urge surfing, breathing into difficult sensations, and the “drop the rope” metaphor in struggles with inner experiences. These are often central in chronic pain, cravings, panic, shame, grief, and trauma-related avoidance.
Defusion Exercises
These target the literal grip of thoughts. Examples include “I’m having the thought that…” saying a difficult thought very slowly, repeating a word until it becomes a sound, “Leaves on a Stream,” and naming recurring stories.
One of the most recognizable defusion exercises is Leaves on a Stream, in which clients imagine placing each thought, image, memory, or feeling onto a leaf that floats by on a gently flowing stream.
Values Clarification Exercises
These target motivational direction. Examples include life-domain values mapping, “What do you want your life to stand for?” regret-to-values reflection, and eulogy or future-self exercises. Values work in ACT is embedded in functional case formulation rather than treated as motivational decoration.
Committed Action and Behavioral Practice
These target action in the real world. Examples include weekly values-aligned goals, graded exposure or activity scheduling, re-engagement plans, barriers-and-skills planning, and if-then implementation statements. This is where therapy succeeds or fails, as psychological flexibility ultimately shows up in what a person does.
Digital and Online ACT
ACT has expanded far beyond traditional face-to-face therapy. A 2020 transdiagnostic meta-analysis of internet-based ACT across 25 studies found small pooled posttreatment effects for anxiety, depression, quality of life, and psychological flexibility, with effects maintained at follow-up.
Critically, therapist-guided internet ACT appeared to produce stronger effects than unguided delivery.
A 2016 systematic review and meta-analysis of 10 randomized controlled trials concluded that web-delivered ACT was effective for depression, with high adherence and completion overall, suggesting good acceptability. The same review found a small effect size for depression, anxiety effects that approached a small-effect threshold, but no effectiveness for quality of life.
Digital ACT is promising precisely because ACT’s techniques are portable. But its long-term effectiveness likely depends on preserving functional guidance, not merely digitizing worksheets.
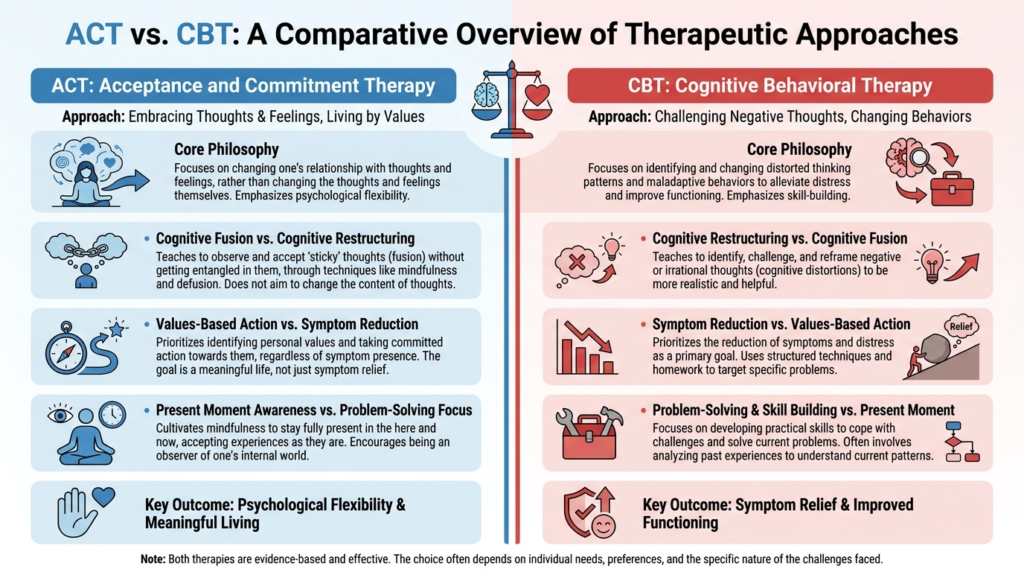
ACT Compared With CBT and Other Approaches
ACT and CBT share a behavioral-cognitive lineage. Both are structured, skills-focused, and empirically oriented.
The difference lies mainly in what each tries to change first. Traditional CBT often targets distorted cognitions, maladaptive beliefs, and avoidance behaviors. ACT often targets cognitive fusion, experiential avoidance, disconnection from values, and inflexible attention.
In CBT, a thought may be examined for evidence and accuracy. In ACT, a thought may be examined for workability and function.
A 2014 meta-analysis of 39 randomized controlled trials concluded that ACT is more effective than treatment as usual or placebo and may be as effective as established psychological interventions for anxiety disorders, depression, addiction, and somatic health problems.
The evidence does not support inflated claims that ACT outperforms all alternatives. What it supports is more interesting and more clinically useful: ACT is one of the most versatile and implementation-ready process-based therapies available, and its comparative strength lies less in universal superiority and more in its fit for complex, comorbid, functionally impairing conditions where rigid control strategies have become part of the problem.
Strengths and Limitations of ACT
Strengths
ACT techniques are not random; they are tied to a unified model of psychological flexibility grounded in Relational Frame Theory and functional contextualism. The same processes recur across depression, anxiety, trauma, chronic pain, and adjustment to injury or illness.
ACT can be used in groups, individual treatment, telehealth, workshops, and digital interventions. It is especially well suited for chronic pain, trauma-related avoidance, and conditions where symptom elimination is incomplete or unrealistic.
ACT frequently improves functioning, coping, and valued action even when symptom reduction is moderate rather than dramatic.
Limitations
ACT often performs similarly to established treatments rather than consistently better. Recent military meta-analysis found significant benefit but with substantial heterogeneity. In traumatic brain injury, ACT did not improve rehabilitation participation or physical health-related quality of life.
When stripped from case formulation, ACT exercises can be used mechanically or as covert symptom-control strategies. Some areas rely on small studies, single-arm designs, or implementation work that needs larger replication.
Who Can Benefit Most From ACT?
ACT may be especially worth considering if you feel stuck fighting your thoughts or feelings, have depression with withdrawal and rumination, find that anxiety keeps shrinking your life, want therapy focused on meaning and action rather than only symptom analysis, or prefer a framework that does not require you to “win” against your mind before living.
For clinicians, ACT is especially useful when experiential avoidance is central, cognitive restructuring is not producing behavior change, values clarification can mobilize action, a transdiagnostic approach is needed, or digital or group-based delivery is desirable.
The overall conclusion is concrete: ACT is a credible, theoretically coherent, and broadly useful psychotherapy whose main strength lies not in replacing CBT, but in offering a process-based alternative especially well suited for chronic distress, transdiagnostic problems, and scalable digital care.
If you’re struggling with difficult thoughts and feelings that seem to control your life, we’re available for help. Contact our team to learn how our evidence-based therapy can support your journey toward greater psychological flexibility and meaningful living.

