You maintain a demanding career, show up for family obligations, and keep your schedule packed. Yet beneath that polished exterior, intrusive memories, hypervigilance, and emotional numbness quietly erode your well-being.
This is high-functioning PTSD: a pattern in which trauma-related symptoms persist while outward role performance remains intact. Research shows that approximately 9.3% of trauma-exposed individuals meet full PTSD criteria, while another 23.7% experience subthreshold symptoms that still cause significant distress.
This article explains how high-functioning PTSD presents, why it often goes undetected, and how it relates to complex PTSD under the ICD-11 framework.
What is High-Functioning PTSD?
High-functioning PTSD is not a formal diagnosis but a clinically recognized pattern. It describes people who meet or nearly meet diagnostic criteria for post-traumatic stress disorder while sustaining outward roles at work, school, or in relationships.
The key is understanding that impairment exists but is displaced or concealed through compensatory strategies like perfectionism, rigid routines, and safety behaviors.
Both DSM-5-TR and ICD-11 require functional impairment for a PTSD diagnosis. DSM-5-TR defines PTSD with six core criteria, including clinically significant distress or impairment in social, occupational, or other important areas.
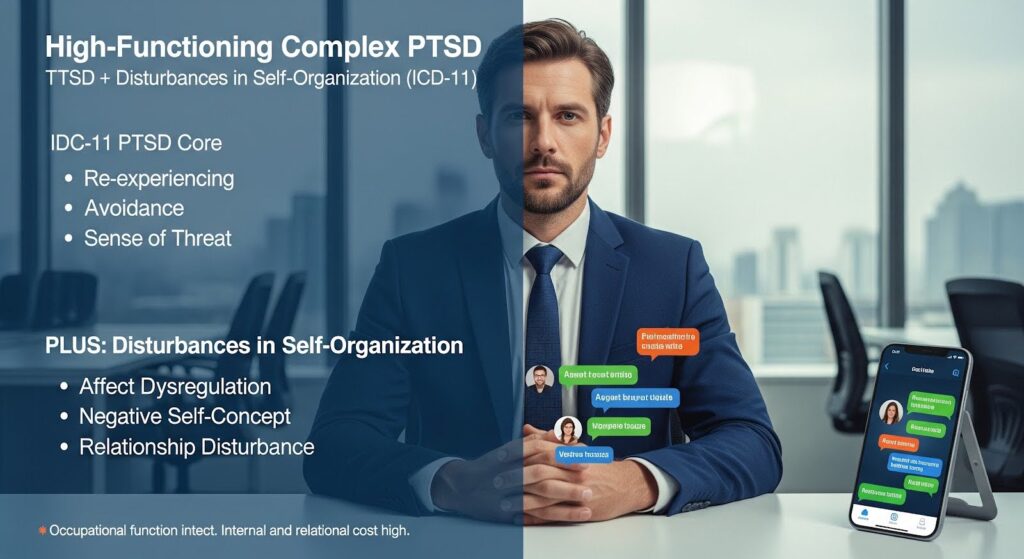
ICD-11 streamlines PTSD to three core symptom types: re-experiencing in the present, deliberate avoidance, and a current sense of threat, each requiring at least one symptom and explicitly requiring functional impairment.
The seeming contradiction resolves when we measure impairment where it actually lives: in sleep fragmentation, relational detachment, cognitive load from hypervigilance, medical utilization for somatic symptoms, and restricted activities.
ICD-11’s framework positions complex PTSD as a separate diagnosis requiring PTSD plus disturbances in self-organization, which include affect dysregulation, negative self-concept, and disturbances in relationships.
Signs of High-Functioning PTSD
Avoidance Disguised as Discipline
Avoidance is a core PTSD feature, but in high-functioning individuals it often appears as productivity. You might stay late at work to avoid quiet time where intrusions surface, delegate tasks that trigger sensory reminders, or maintain rigid schedules that incidentally sidestep trauma cues.
These behaviors work in the short term by minimizing intrusions, but life space shrinks and spontaneity dies off.
Hypervigilance Mistaken for Drive
The PCL-5 assessment tool captures irritability, hypervigilance, exaggerated startle, concentration problems, and sleep disturbance. These features can look like Type A drive or high-alert conscientiousness.
Differentiation hinges on trauma linkage: Are lapses in concentration triggered by trauma cues? Do symptoms intensify with trauma reminders and ease with avoidance? In high-demand roles, hypervigilance can be rewarded, obscuring its pathological underpinnings and cost.
Emotional Numbing as Professionalism
Emotional numbing often appears as reduced intimacy and self-disclosure, explained away as being busy or guarded. You maintain surface competence in social roles but feel detached in deeper ties. Partners describe a flatness or constrained affect, a sense of being there but not present.
These are material impairments, especially in ICD-11 complex PTSD where relationship disturbances and negative self-concept are core features, but they are commonly missed when patients emphasize work functioning.
Sleep Disturbance as a Hidden Driver
Sleep fragmentation and nightmares sustain daytime fatigue, irritability, inattention, and somatic pain sensitivity. High-functioning individuals may cope via increased caffeine, rigid routines, and workaholism.
Without sleep-focused inquiry, impairment is displaced from work output to long-term health costs and relational strain.
High-Functioning PTSD Symptoms vs. Other Conditions
PTSD and ADHD Overlap
Concentration problems, restlessness, irritability, and sleep disturbance can look ADHD-like. Key guardrails include developmental onset: ADHD requires symptom presence before age 12 across settings, while PTSD symptoms by definition follow trauma exposure.
PTSD-related inattention is cue- and state-dependent, often fluctuating with avoidance and arousal, whereas ADHD is more trait-like and cross-situational.
PTSD and OCD Similarities
PTSD and OCD share intrusions, avoidance, and safety behaviors. In high-functioning PTSD, trauma-linked compulsions like checking locks in a pattern, scanning exits, or excessive cleaning of specific cues can be misread as OCD.
Distinguish by intrusion content: Is the obsession-like thought directly connected to a traumatic event? Is the behavior aimed at reducing trauma-specific threat rather than neutralizing unacceptable thoughts? Joint assessment is often required given notable comorbidity.
Somatic Presentations
PTSD is associated with elevated migraine prevalence, and migraineurs show higher odds of PTSD than those without headache.
Somatic comorbidity is a hallmark of high-functioning PTSD: individuals may present repeatedly for medical complaints like headaches or GI symptoms without concurrent mental health disclosure. Screening for PTSD in high-frequency somatic care users can unmask hidden trauma-linked psychopathology.
What is High-Functioning Complex PTSD?
Complex PTSD represents a distinct sibling diagnosis to PTSD in ICD-11. It requires PTSD plus disturbances in self-organization: pervasive and persistent difficulties in affect regulation, negative self-concept, and disturbances in relationships, with functional impairment explicitly tied to these features.
Studies comparing ICD-11 PTSD and complex PTSD reveal that complex PTSD is generally more severe, with elevated maladaptive personality traits, especially Negative Affectivity and Psychoticism. These traits amplify vulnerability to relational dysfunction, shame and guilt cycles, and social withdrawal, which are hallmarks of masked impairment outside the workplace.
High-functioning complex PTSD often presents with well-maintained occupational performance that conceals heavy internal distress and specific impairments in intimacy, identity, and social participation.
Because complex PTSD explicitly encodes disturbances in self-organization with associated functional impairment, it can detect clinically important interpersonal and self-concept difficulties even when occupational functioning is preserved.
- Affect dysregulation: Difficulty managing emotional responses, swinging between hyperactivation and emotional numbing
- Negative self-concept: Persistent feelings of worthlessness, shame, or failure
- Relationship disturbances: Difficulty feeling close to others or maintaining intimate connections
How People Mask PTSD Symptoms?
Task-Focused Avoidance
Intensive engagement in work or projects provides structure, distraction from intrusions, and a sense of safety and control. This reinforces avoidance while yielding social validation as productive and reliable.
The strategy can obscure underlying hyperarousal, sleep disturbance, or emotional numbing in professional contexts.
Perfectionism and Overcontrol
Rigid orderliness and compulsive standards minimize uncertainty and threat but can produce indecision and inefficiency when stakes feel high.
Research on obsessive-compulsive personality disorder shows that OCPD tendencies are not equivalent to healthy conscientiousness and can even inversely relate to it, reflecting perseveration and impaired task completion under stress. Apparent high function may be brittle and situational.
Compartmentalization Across Life Domains
Large-sample psychometric research shows that dysphoric PTSD symptom clusters, such as anhedonia and dysphoric arousal, exhibit the strongest associations with psychosocial functioning.
In high-functioning cases, impairment may concentrate in non-work domains like family, intimacy, and community, with dysphoric features either partially concealed or transiently compensated in professional tasks.
Detecting High-Functioning PTSD
Screening with PC-PTSD-5
The 5-item PC-PTSD-5 screener performs robustly in primary care settings. In a veteran primary care sample, it achieved excellent accuracy with an AUC of 0.941. A cut score of 3 maximizes sensitivity while maintaining specificity above 0.80, identifying 94.8% of PTSD cases.
For primary care detection where missing cases is costly, a cut of 3 is typically optimal, with follow-up assessment to resolve false positives.
Severity Assessment with PCL-5
The PCL-5 is a 20-item, DSM-5-aligned, validated instrument used for provisional PTSD status and symptom severity. Common cutoffs for probable PTSD range from 31 to 33, balancing sensitivity and specificity across many populations.
However, optimal cutoffs vary substantially by population, setting, and goal. Continuous scores help monitor masked symptom change even when categories stay constant.
Phenotyping with the International Trauma Questionnaire
The International Trauma Questionnaire is the primary standardized instrument for ICD-11 PTSD and complex PTSD. It includes 18 items covering PTSD symptoms, disturbances in self-organization, and functional impairment.
The ITQ permits both categorical diagnosis and dimensional severity scoring, making it well-suited to capture subclinical or high-functioning patterns and to differentiate PTSD from complex PTSD in routine care.
Measuring Functional Impairment
Domain-based measures detect clinically meaningful change even when symptom totals fluctuate minimally. The WHO Disability Assessment Schedule 2.0 measures functioning across six domains: cognition, mobility, self-care, getting along, life activities, and participation.
Among veterans seeking PTSD compensation, WHODAS and the Inventory of Psychosocial Functioning were stronger indicators of functioning than the Global Assessment of Functioning scale.
The Sheehan Disability Scale is a brief 3-item measure covering work or school, social life, and family or home, yielding 0 to 10 ratings per domain.
Scores of 5 or higher in any domain merit attention. SDS is useful to rapidly capture the cost of masking, such as high work function but severe social or family impairment.
A Practical Detection Approach
Step 1: Screen inclusively
Use PC-PTSD-5 with a cut score of 3 or higher in general primary care. Consider a cut of 2 or even 1 in high-risk, underrepresented, or socioeconomically vulnerable settings where missed cases have high costs and stigma may suppress disclosure.
Step 2: Confirm and quantify severity
Administer PCL-5 and interpret cutoffs contextually, around 34 for clinical case-finding. Pay extra attention to dysphoric clusters like anhedonia and dysphoric arousal, which strongly predict functional impairment. Ask explicitly about concentration, fatigue, sleep, and loss of interest even if work output seems stable.
Step 3: Phenotype with ICD-11 ITQ
Use the ITQ to differentiate PTSD versus complex PTSD. Score both categorically and dimensionally. Probe disturbances in self-organization items for patterns of hyper or hypo activation, pervasive negative self-concept, and relational disturbances. Explicitly document functional impairment linked to these features, even in the presence of intact occupational function.
Step 4: Measure function to unmask cost
Administer WHODAS 2.0 to quantify domain impairments. Track minimal important differences of approximately 3 points for the 12-item version to confirm meaningful change. In brief visits, use the Sheehan Disability Scale to capture work, social, and family costs.
Step 5: Consider differential diagnosis
Screen for borderline personality disorder features, dissociation severity, and trauma-related maladaptive beliefs. If strong disturbances in self-organization with trauma-linked beliefs and less pronounced dissociation instability, complex PTSD is likely. Use structured or semi-structured tools where possible and maintain a trauma-informed stance.
Treatment Considerations
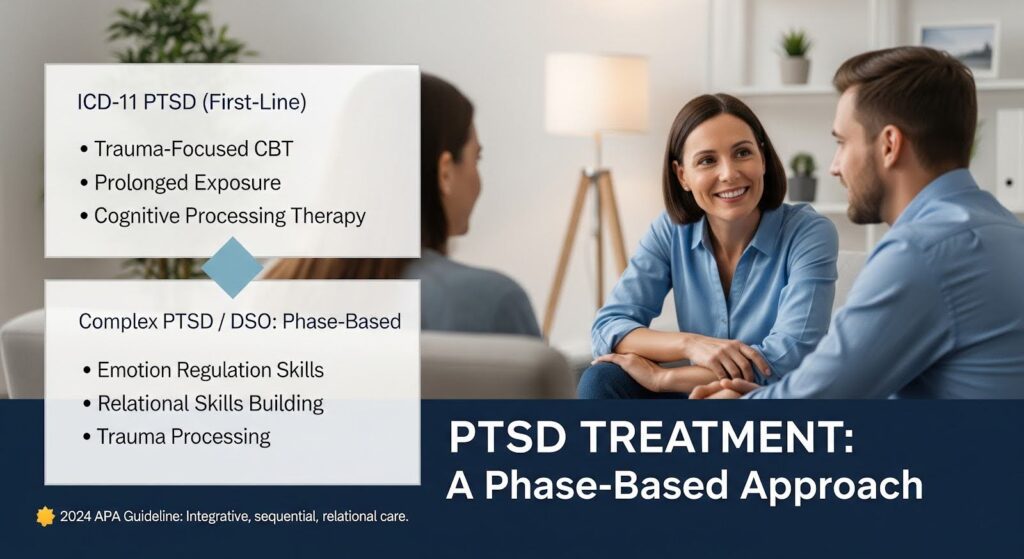
PTSD-focused therapies like trauma-focused cognitive behavioral therapy, prolonged exposure, and cognitive processing therapy remain first-line for ICD-11 PTSD, targeting fear-based memory processes and maladaptive beliefs.
For complex PTSD or PTSD with prominent disturbances in self-organization, meta-analytic and conceptual reviews suggest phase-based or multimodal interventions may be advantageous, such as emotion regulation and relational skills building before or alongside trauma processing.
The 2024 APA Professional Practice Guideline for Working with Adults with Complex Trauma Histories emphasizes trauma-informed, humanistic, integrative, sequential, relational, and outcomes-focused care. These principles align with disturbances in self-organization focused work and with the need to assess functional change, not just symptom reduction.
For high-functioning presentations, normalize and validate masking by framing perfectionism and workaholism as understandable safety strategies that carry hidden costs. Collaboratively explore values-driven exposure to intimacy and participation.
Use functioning measures to show the cost ledger of masking, such as social avoidance equaling moderate disability, thereby justifying targeted work on self-organization.
Why Does it Matter?
High-functioning PTSD is common precisely because modern life provides structures like rigid schedules, high-demand roles, and digital communication that permit avoidance, overcontrol, and hypervigilance to masquerade as conscientiousness and productivity.
Unless we measure trauma linkage and the costs in sleep, intimacy, spontaneity, and health utilization, we will systematically miss these cases.
The ICD-11 PTSD and complex PTSD framework, operationalized via the International Trauma Questionnaire and combined with flexible severity tools and domain-based functioning measures, offers the most clinically actionable pathway to detect and treat high-functioning PTSD.
This approach directly measures the disturbances in self-organization most likely to be hidden behind occupational success and allows clinicians to document and track the concealed disability where patients live: in relationships, self-worth, and social participation.
If you recognize these patterns in yourself or someone you care about, know that effective, evidence-based treatment exists. You don’t have to keep carrying the weight alone while maintaining the appearance of having it all together.
So, reach out to explore Summit’s trauma therapy in Atlanta and begin the process of healing beneath the surface.

