Separation anxiety in adults is a real and often underrecognized anxiety disorder marked by excessive fear and distress when away from important attachment figures such as a spouse, partner, parent, or child. Many adults first develop these symptoms later in life rather than in childhood.
This article explains what adult separation anxiety looks like, what causes it, and how evidence-based treatment can help you regain independence and emotional stability.
What is Separation Anxiety in Adults?
Adult separation anxiety disorder involves developmentally inappropriate and excessive fear or anxiety about being separated from major attachment figures.
Unlike normal concern for loved ones, this condition causes clinically significant distress and impairment in daily functioning. The DSM-5 reclassified separation anxiety among anxiety disorders and removed the previous requirement that symptoms begin before age 18, formally recognizing that adults can develop this condition for the first time in adulthood.
In adults, the attachment figure may be a romantic partner, spouse, parent, or child rather than a caregiver in the childhood sense. The disorder requires at least three characteristic symptoms persisting for six months or longer, along with clinically significant distress or functional impairment.
How Common is Adult Separation Anxiety?
Research shows that adult separation anxiety is more prevalent than previously assumed. Lifetime prevalence across countries is approximately 5%, with U.S. adult lifetime prevalence reported at 6.6%. In clinical outpatient samples, roughly 20% to 23% of adults with anxiety or mood disorders meet criteria for adult separation anxiety disorder.
Importantly, the majority of adult cases represent first onset in adulthood rather than continuation from childhood. Approximately 77.5% of adult cases in the National Comorbidity Survey Replication had first onset in adulthood, challenging the outdated assumption that adult separation anxiety is always unresolved childhood anxiety.
What Causes Separation Anxiety in Adults?
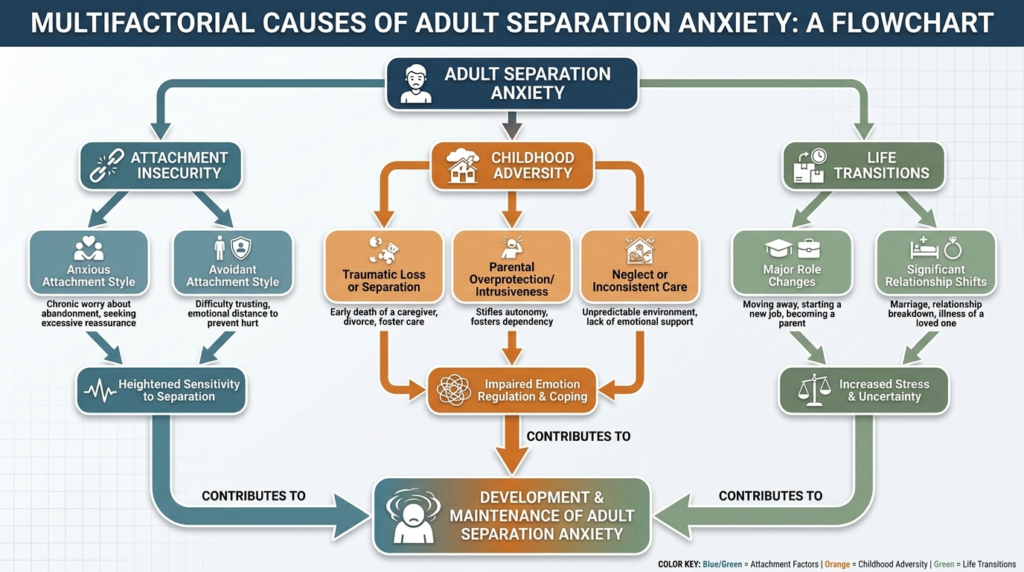
Adult separation anxiety does not have one single known cause. Rather, it emerges from the interaction of multiple vulnerability factors across developmental, psychological, and environmental domains.
Attachment Insecurity
Attachment theory provides one of the most influential frameworks for understanding adult separation anxiety. Insecure attachment patterns, especially anxious attachment, are significantly associated with adult separation anxiety symptoms.
When prior caregiving was inconsistent, threatening, or insufficiently containing, separation from attachment figures can activate intense distress.
Research in emerging adults found that adult separation anxiety symptoms were significantly associated with anxious attachment, with indirect links from childhood separation anxiety memories to adult attachment through current adult separation anxiety.
Childhood Adversity and Trauma
Cross-national WHO data found that maladaptive family functioning childhood adversities and other childhood adversities were associated with separation anxiety disorder onset. Importantly, these adversities predicted not only pediatric-onset but also adult-onset separation anxiety disorder.
A 28-year study of children exposed to a major bushfire found that brief separation from parents during trauma predicted more avoidant attachment in adulthood, and adult attachment insecurity in turn related to PTSD symptom clusters. This suggests that separation in threatening contexts may contribute specifically to later attachment insecurity and psychopathology.
A 2023 study found adult separation anxiety associated with cognitive distortions involving negative self-image, self-blame, helplessness, hopelessness, and preoccupation with danger. Helplessness and danger preoccupation fully mediated the relationship between childhood sexual abuse and adult separation anxiety.
Family Dysfunction and Overprotective Caregiving
Clinical and research sources consistently identify several family-related risk factors:
- Overprotective or anxious caregiving
- Family history of anxiety disorders
- Inconsistent caregiving
- Childhood anxiety disorders
- Major losses or disruptions in early life
Familial and Genetic Contributions
A 2022 family study concluded that parental adult separation anxiety is an important, though non-specific, risk factor for children’s psychopathology.
The pathway may be genetic, environmental, or include child-to-parent effects. This suggests broader internalizing liability may be transmitted, with separation anxiety as one manifestation.
Life Transitions and Stressors
Adult-onset separation anxiety often emerges during developmental transitions such as:
- Leaving home for the first time
- Marriage or new romantic relationships
- Moving to a new city
- Pregnancy or becoming a parent
- Relationship loss or divorce
- Caregiving stress for aging parents
- Bereavement or traumatic loss
A Multifactorial Model
The most evidence-based understanding is that adult separation anxiety emerges from the interaction of early adversity, attachment insecurity, inherited internalizing temperament, later stress or trauma, cognitive distortions, and avoidance patterns that maintain the disorder over time.
Why Adult Separation Anxiety is Often Missed?
Adult separation anxiety has been historically underdiagnosed. Before DSM-5, adults with separation anxiety symptoms were often classified under panic disorder, agoraphobia, or generalized anxiety disorder. Diagnostic rules implied it was a childhood condition, and clinicians often overlooked it in adults.
Differential Diagnosis
Adult separation anxiety overlaps with multiple disorders, making accurate diagnosis challenging:
Panic disorder and agoraphobia: Fear of being away from safety or help can resemble agoraphobia, but in separation anxiety the feared catastrophe is especially linked to attachment loss or distance from attachment figures.
Generalized anxiety disorder: Adults with GAD worry broadly about many life domains, while separation anxiety worry is more specifically organized around separation and attachment figures.
PTSD and trauma-related conditions: Trauma history can produce hypervigilance, fear of loss, and attachment dysregulation. Trauma may contribute causally to adult separation anxiety, but the syndromes are not identical.
Dependent personality features: Reliance on others and fear of separation may overlap with personality structure, but adult separation anxiety has a more clearly anxiety-based symptom pattern, often episodic or stress-reactive.
Clinical Clues
Several clinical clues suggest separation anxiety may be the hidden driver:
- Refractory anxiety or poor response to standard treatment
- Panic-agoraphobic symptoms that worsen when alone
- Chronic reassurance-seeking in close relationships
- Disproportionate distress when attachment figures are unavailable
- Inability to perform independent tasks despite intact ability
- Sleep disturbance related to proximity
One study of adult anxiety treatment nonresponders found that 80% met the threshold for clinically significant separation anxiety symptoms, suggesting that separation anxiety may be a major but underrecognized factor in refractory adult anxiety presentations.
Treatment Options for Separation Anxiety in Adults
The strongest treatment conclusion supported by available evidence is that cognitive behavioral therapy, especially when it includes graded exposure and cognitive restructuring, should currently be considered the most practical first-line treatment framework for adults with separation anxiety.
Cognitive Behavioral Therapy
CBT is repeatedly described as a first-line treatment for most anxiety disorders and is strongly supported across adult anxiety presentations. Core CBT elements such as exposure and cognitive restructuring have the strongest backing across anxiety disorders.
Core CBT components for adult separation anxiety include:
Psychoeducation: Patients learn that separation anxiety can occur in adults, distress is anxiety-based rather than proof of actual danger, avoidance temporarily relieves anxiety but maintains the disorder, and tolerance of separation can be relearned through practice.
Cognitive restructuring: This targets catastrophic beliefs such as “If I’m not there, something terrible will happen,” “If I’m alone, I won’t cope,” or “Distance means abandonment.” CBT identifies these distortions, gathers evidence for and against them, and tests alternative explanations.
Graded exposure: This is the central behavioral treatment mechanism. Patients gradually face feared situations while reducing avoidance, distraction, and safety behaviors. For adult separation anxiety, exposures might include staying home alone briefly, going on a short solo walk, delaying reassurance texts, sleeping alone for part of the night, completing errands independently, or spending increasing planned periods apart from the attachment figure.
Reducing safety behaviors: Exposure works best when the person does not neutralize the feared situation with safety behaviors such as constant texting or calling, tracking the loved one’s location, insisting on accompaniment, or seeking repetitive reassurance.
Relapse prevention: Planning for future high-risk situations such as travel, relationship conflict, illness, or moves helps maintain gains after active treatment ends.
Exposure Therapy: The Most Important Practical Tool
If one intervention component deserves emphasis above all others, it is graded real-life exposure. Exposure is essential, should be graded, should occur in-session and between sessions, should reduce avoidance and safety behaviors, and works in part by habituation and disconfirmation of feared consequences.
A graded exposure hierarchy might include:
- Spending 5 minutes in another room without texting partner
- Walking alone for 10 minutes without calling to check in
- Grocery shopping alone without live location monitoring
- Staying home alone for 1 hour without repeated phone checking
- Sleeping separately one night or part of night
- Spending half a day apart with planned check-in only
- Full day apart engaged in independent activities
- Short solo trip or overnight separation
Pharmacotherapy
Medication may be considered for severe or comorbid cases, but the disorder-specific pharmacotherapy evidence in adults is limited and still emerging. A randomized controlled pilot trial investigated vilazodone for adult separation anxiety disorder, suggesting that medication research is emerging but not yet well established.
SSRIs are plausible options, especially by extrapolation from anxiety treatment and older separation anxiety disorder reviews, but current evidence does not justify presenting medication as the leading treatment modality for adult separation anxiety.
Medication should be considered an adjunct or selective option when symptoms are severe, comorbidity is substantial, psychotherapy response is partial, or distress is too intense to engage well in exposure.
Attachment-Focused Psychotherapy
An attachment-focused psychodynamic intervention showed promise in a small open trial among anxiety treatment nonresponders with high separation anxiety symptoms. Over 21 to 24 sessions across 12 weeks, patients showed improvements in current separation anxiety, overall anxiety severity, and global severity.
This suggests that in some refractory patients, attachment dynamics are central, and an attachment-focused approach may be useful when standard CBT or medication has not adequately addressed the separation-based core.
Signs and Symptoms of Separation Anxiety in Adults
Adult separation anxiety presents differently than childhood separation anxiety, though the core fear remains similar. Adults often focus on spouses, romantic partners, children, or elderly parents rather than caregivers.
Core Symptoms
According to DSM-5-TR criteria, adults with separation anxiety disorder typically experience at least three of the following symptoms:
- Excessive distress during or in anticipation of separation from attachment figures
- Persistent worry that harm will come to the attachment figure
- Worry that something will happen to oneself leading to separation, such as illness or accident
- Reluctance or refusal to leave home, go to work, or travel due to fear of separation
- Fear of being alone or without the attachment figure nearby
- Difficulty sleeping without proximity to the attachment figure or sleeping away from home
- Nightmares with separation themes
- Physical symptoms such as nausea, headaches, stomach distress, or vomiting when separation occurs or is anticipated
How Adult Symptoms Differ From Childhood Presentations?
While children more often fear separation from parents and show visible behavioral protest, adults may exhibit subtler but equally impairing patterns. These include repeated reassurance seeking, refusal of travel, inability to sleep alone, work avoidance, or organizing life around minimizing separation.
Adults may become intensely anxious when away from a spouse or partner, panic when their partner leaves for business travel, refuse overnight travel because they fear a parent may die while they are away, or avoid independent activities because being apart from an attachment figure feels intolerable.
Real-Life Examples
Adult separation anxiety may look like:
- A parent who cannot go to work without repeatedly checking whether their child is safe
- A spouse who experiences panic-like symptoms when their partner travels
- An adult child who refuses work opportunities requiring relocation due to fear of being far from aging parents
- A person who sleeps poorly unless a partner is physically present in the bed
- Someone who avoids medical appointments, errands, or social activities that require being alone

Self-Management and Coping Strategies
While professional treatment is essential for clinically impairing cases, structured coping strategies are important adjuncts.
Practice Planned Separations
Schedule separations rather than waiting for unavoidable ones. Start with 5 minutes alone, then 10, then 30, then a full errand, then longer periods. This builds mastery instead of panic.
Limit Reassurance Frequency Intentionally
Set rules such as one planned check-in instead of multiple unscheduled texts, no immediate second message if there is no reply, and no location checks unless truly necessary. The goal is reducing compulsive reassurance loops.
Track Catastrophic Thoughts
Write down the feared outcome, the predicted probability, what happened, and what you learned. This transforms vague dread into testable predictions.
Use Mindfulness to Stay Present
During separation, notice the body, breathe slowly, label the feeling as anxiety rather than danger, and remain in the situation until the wave passes. Mindfulness, meditation, yoga, and deep breathing help lower acute autonomic arousal and improve tolerance of uncertainty.
Build a Structured Day
Prepare tasks, exercise, meals, enjoyable activities, and social contact not centered on the attachment figure. Unstructured waiting tends to magnify distress.
Develop Identity Outside the Attachment Relationship
Hobbies, work roles, friendships, volunteering, learning goals, and solo routines matter because they reduce the dominance of the attachment system over the whole self.
Self-Care Foundations
Daily self-care basics such as exercise, healthy eating, and adequate sleep reduce symptom intensity and improve stability. These strategies reduce physiologic vulnerability to anxiety and improve emotional resilience.
Building Emotional Independence
Adult separation anxiety often persists because the environment unintentionally reinforces it. A partner may repeatedly reassure, remain constantly available, modify routines to avoid triggering distress, or tolerate escalating monitoring. These accommodations usually come from care, but they can stabilize the disorder.
Key targets in autonomy-building include:
- Reduce excessive reassurance-seeking
- Tolerate delayed responses
- Increase solo functioning
- Expand sources of social support
- Cultivate personal interests and roles independent of the attachment figure
- Establish healthy relationship boundaries
For many adults, the most meaningful clinical improvement occurs when the person regains independent functioning, not merely when anxiety feels lower.
Treatment goals should include going places alone, sleeping independently when appropriate, reducing compulsive contact, tolerating uncertainty, and reclaiming work, social, and personal roles.
When to Seek Professional Help?
You should consider professional evaluation if:
- Separation-related anxiety persists for six months or longer
- Distress is excessive relative to the situation
- Symptoms interfere with work, relationships, or daily activities
- You avoid important activities due to fear of separation
- Physical symptoms such as nausea, headaches, or sleep disturbance are frequent
- Reassurance-seeking or checking behaviors are compulsive
- Previous anxiety treatment has not adequately helped
A psychiatric or qualified mental health evaluation should identify the attachment figures, symptom triggers, avoidance patterns, reassurance-seeking, safety behaviors, functional impairment, relationship dynamics, and co-occurring anxiety, mood, trauma, or obsessive-compulsive symptoms.
Why Does It Matter?
Adult separation anxiety is not simply being clingy or missing someone a lot. Reviews emphasize that it is associated with clinically significant distress and severe impact on functioning.
Adults may struggle with leaving home, tolerating solo errands or travel, sleep independence, work attendance or advancement, relocation, marriage-related autonomy shifts, tolerating normal distance in close relationships, and functioning as an independent adult.
The clinical significance of this impairment is amplified by its tendency to blend into relationship dynamics. Excessive check-ins, demands for proximity, inability to tolerate delayed replies, or insistence on accompaniment may gradually strain relationships, reinforce dependency, and limit personal development.
Conclusion
Adult separation anxiety is a real, clinically meaningful, and underrecognized anxiety disorder that cannot be dismissed as either normal attachment or merely a leftover childhood condition.
The most persuasive research shows that it can begin in childhood and persist, but it can also emerge for the first time in adulthood, especially in the context of attachment vulnerability, adversity, trauma, or major life stress.
The most effective current strategy for treating and managing separation anxiety in adults is a CBT-centered approach that explicitly targets separation-based catastrophic beliefs, avoidance, reassurance-seeking, and safety behaviors through graded real-life exposure and cognitive restructuring, while simultaneously strengthening daily stability through sleep, exercise, routine, mindfulness, and broader support.
If you or someone you care about is struggling with excessive fear of separation, difficulty being alone, or relationship patterns that limit independence, know that effective help is available. With the right support and evidence-based treatment, adults with separation anxiety can regain autonomy, strengthen relationships, and build a more confident, independent life.
If you’re ready to take the next step toward managing separation anxiety and reclaiming your independence, reach out to our team to learn how compassionate, evidence-based care can help.

