Attachment therapy addresses one of the most fundamental aspects of human development: the bonds we form with caregivers in early life.
These early relationships don’t just shape childhood, they influence how we regulate emotions, trust others, and navigate relationships throughout our lives. When attachment goes wrong, the effects can ripple through decades, affecting mental health in ways that standard treatments often miss.
This article explains what attachment therapy is, how attachment patterns affect mental health, and which therapeutic approaches show the strongest evidence for healing attachment wounds.
What Attachment Therapy Actually Means?
The term “attachment therapy” requires immediate clarification. Mainstream clinical sources warn that attachment-based therapy should not be confused with harmful practices historically labeled “attachment therapy” that involved restraint, deprivation, or coercive methods.
Legitimate attachment-based therapy is grounded in attachment theory and uses non-coercive, evidence-informed approaches to address relational trauma and insecure attachment patterns.
Attachment-based therapy refers to psychotherapies informed by attachment theory, the developmental framework established by John Bowlby in the 1950s and 1960s. Bowlby’s core insight was that attachment is a primary motivational system organized around proximity to protective caregivers, not a secondary byproduct of feeding or gratification.
His work, detailed in the *Attachment and Loss* trilogy published between 1969 and 1980, linked early caregiver bonds, separation, and loss to later emotional development and psychopathology.
Several key concepts from Bowlby’s work became foundational to psychotherapy. The secure base concept describes how safety in a caregiver relationship supports exploration, confidence, and emotional regulation.
Internal working models are organized expectations about self, others, and relationships shaped by attachment experience. These models help explain repetitive interpersonal patterns, shame, mistrust, and defensive strategies that persist into adulthood.
Core Principles of Attachment-Based Work
Despite the diversity of specific modalities, legitimate attachment-based therapies share several recurring principles:
- The therapeutic relationship functions as a secure base through which clients can explore trauma and develop more secure relational patterns
- Attunement and co-regulation address dysregulation in relational contexts rather than through cognitive reinterpretation alone
- Repair of attachment ruptures restores trust, safety, and communication in relationships
- Narrative integration helps clients construct coherent meaning from fragmented or shame-laden experiences
- Reflective function and mentalizing increase the capacity to understand one’s own and others’ mental states under emotional stress
How Attachment Trauma Develops and Affects Mental Health?
Attachment trauma refers to trauma arising within primary attachment relationships when those relationships are characterized by sustained failures of protection, soothing, regulation, and attunement, or ongoing abuse.
Recent conceptual work published in Clinical Neuropsychiatry defines attachment trauma as occurring when a child faces prolonged and severe failures in protection, regulation, and caregiving, or active ongoing abuse, resulting in threats that are recurrent or lasting and cannot be escaped.
This definition distinguishes attachment trauma from single-incident trauma. When the person who should be the source of safety also becomes the source of danger, neglect, or chronic misattunement, the child cannot simply avoid the attachment figure.
The child depends on that figure for survival, creating a paradox of seeking closeness to the very person who is frightening, absent, or dysregulating.
Importantly, attachment trauma includes more than overt maltreatment. Persistent emotional absence, unpredictability, dismissiveness, lack of protection, or failure to help regulate distress can become developmentally traumatic when severe and sustained.
Many adults struggle profoundly despite histories they describe as “not that bad” because chronic relational misattunement itself alters affect regulation, attentional control, and representation of self and others.
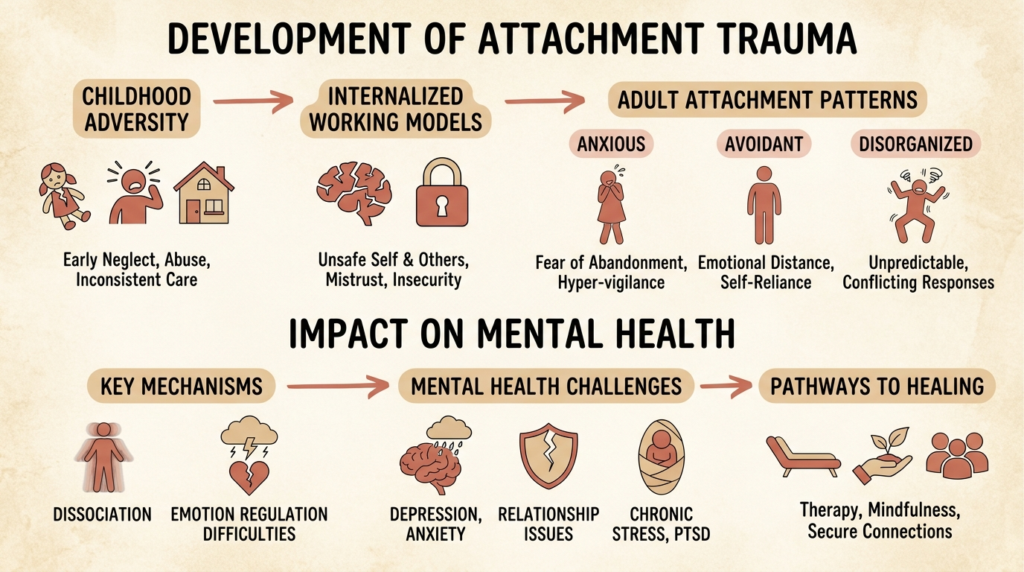
The Link Between Childhood Adversity and Adult Attachment Patterns
A 2026 study published in Frontiers in Psychology examined the relationship between childhood trauma and adult attachment styles using the Adverse Childhood Experiences (ACE) questionnaire and validated adult attachment measures.
The study found a significant relationship between higher ACE scores and greater prevalence of insecure attachment styles. Participants with multiple childhood adversities were more likely to report fear of abandonment, avoidance of intimacy, difficulty with emotional closeness, and trouble trusting others.
Lower ACE scores were linked more often to secure attachment, healthier emotional regulation, and stronger interpersonal trust.
These findings support attachment insecurity as a key pathway through which early trauma affects later relational functioning. However, the most important recent findings go further: childhood adversity does not simply hardwire insecure attachment directly.
A 2024 study summarized in Simply Psychology found that ACEs predicted adult anxious attachment indirectly through both dissociation and emotion regulation difficulties, while ACEs predicted adult avoidant attachment through dissociation but not through emotion regulation difficulties alone.
When dissociation and emotion regulation were included in the analysis, ACEs no longer directly predicted anxious or avoidant attachment.
This means the interpersonal effects of childhood adversity are carried through post-traumatic processes, particularly dissociation and dysregulation, rather than operating as simple direct consequences.
How Attachment Patterns Affect Mental Health Across the Lifespan?
Attachment trauma functions as a transdiagnostic developmental-clinical phenomenon. It does not map neatly onto one disorder but can manifest through multiple symptom domains across diagnostic categories.
A 2025 clinical conceptualization argues that attachment trauma should be identified even when patients do not explicitly report childhood maltreatment, because it may present indirectly through broad psychopathology and difficulties in treatment.
Major domains affected include dysregulation of arousal, emotional and impulse dyscontrol, detachment and dissociative reactions, dysfunctional self and relational representations, impaired mentalization, epistemic mistrust, and maladaptive compensatory strategies.
Broad Mental Health Risk
A systematic review and meta-analysis of prospective longitudinal studies found that ACEs are significant risk factors for multiple adult mental health outcomes. Pooled associations were strongest for PTSD (OR = 2.26), followed by anxiety (OR = 1.78), depression (OR = 1.61), psychotic-like experiences (OR = 1.34), and suicidality (OR = 1.28). Violence or maltreatment-related ACEs were especially associated with depression relative to household ACEs.
A 2022 meta-analysis of 224 studies involving 79,722 participants found that higher attachment anxiety and avoidance were positively correlated with negative mental health indicators and negatively correlated with positive mental health indicators. Attachment avoidance had moderate associations with worse mental health, with anxiety also showing substantial associations.
Common Adult Manifestations
Attachment trauma often appears as recurring constellations of symptoms and relational patterns rather than one neat syndrome.
Anxious-preoccupied patterns may include fear of abandonment, heightened sensitivity to distance or rejection, intense reassurance seeking, difficulty self-soothing, and emotional amplification under relational stress.
Dismissive-avoidant patterns may include discomfort with dependence or vulnerability, distancing from emotional closeness, minimization of needs, compulsive self-reliance, and emotional deactivation or numbing.
Fearful-avoidant patterns may include simultaneous longing for and fear of closeness, unstable relational engagement, mistrust, oscillation between approach and withdrawal, and higher overall self-organization difficulties.
A 2024 scoping review on attachment and somatic symptoms in survivors of childhood trauma suggested that insecure and disorganized attachment orientations are related to DNA damage, metabolic syndrome and obesity, physical pain, functional neurological disorder, and somatization.
This supports a more integrated biopsychosocial view: attachment trauma influences not just thoughts and relationships, but bodily regulation and health pathways as well.
Why Attachment Trauma is Often Missed in Clinical Settings?
Recent clinical literature emphasizes that attachment trauma may need to be identified even when patients do not explicitly report childhood maltreatment.
Reasons include the absence of a single dramatic memory, minimization or normalization of neglect, dissociative barriers to recall, loyalty to caregivers, shame, limited language for early relational deprivation, and confusion between “normal family problems” and trauma.
A patient may say, “I had a normal childhood,” while also reporting chronic emptiness, inability to trust, severe emotional swings in relationships, shutdown under closeness, repeated therapy dropout, and intense reactions to perceived therapist inconsistency. Such a presentation should raise the possibility of attachment trauma even if the history is incomplete.
The 2025 conceptualization work notes that attachment trauma may present indirectly through broad psychopathology and treatment resistance.
If a patient understands their problems intellectually but cannot sustain change, repeatedly mistrusts care, disengages after perceived ruptures, or becomes destabilized by ordinary therapeutic closeness, the issue may not be lack of motivation or insight. It may be that the therapeutic relationship itself activates traumatic internal working models.
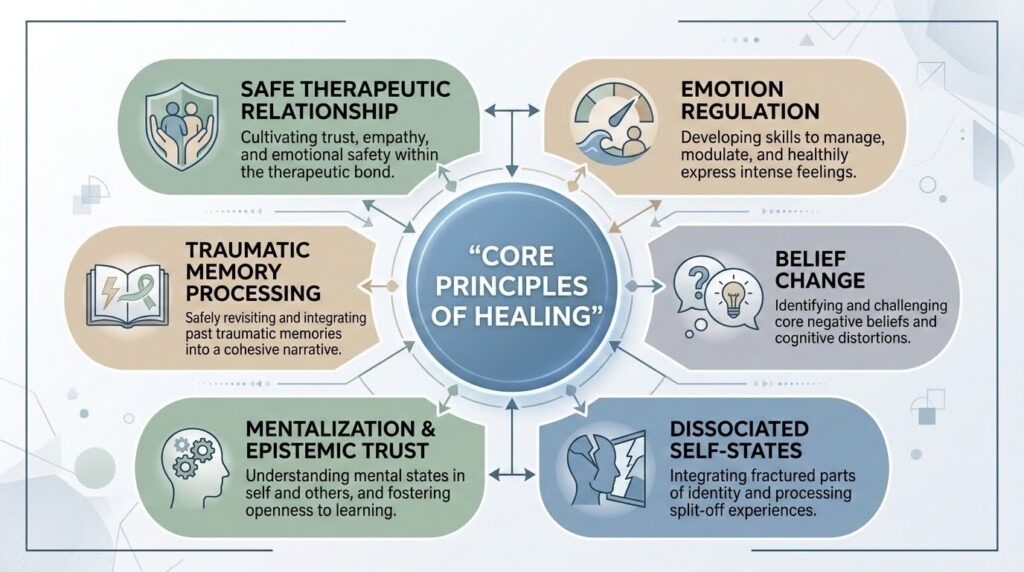
How Therapy Helps: Core Principles of Healing
Among all the evidence reviewed, the most clinically authoritative treatment synthesis is the 2025 paper on psychopathological domains of attachment trauma. It identifies shared therapeutic elements across different modalities:
- Establishment of a safe therapeutic relationship
- Regulation of emotions and arousal
- Modification of pathogenic beliefs
- Addressing detachment symptoms and dissociated self-states
- Promotion of mentalization and epistemic trust
- Processing implicit and explicit traumatic memories
This list is more useful than arguing that one branded therapy is universally best. It identifies the mechanisms treatment must address regardless of modality.
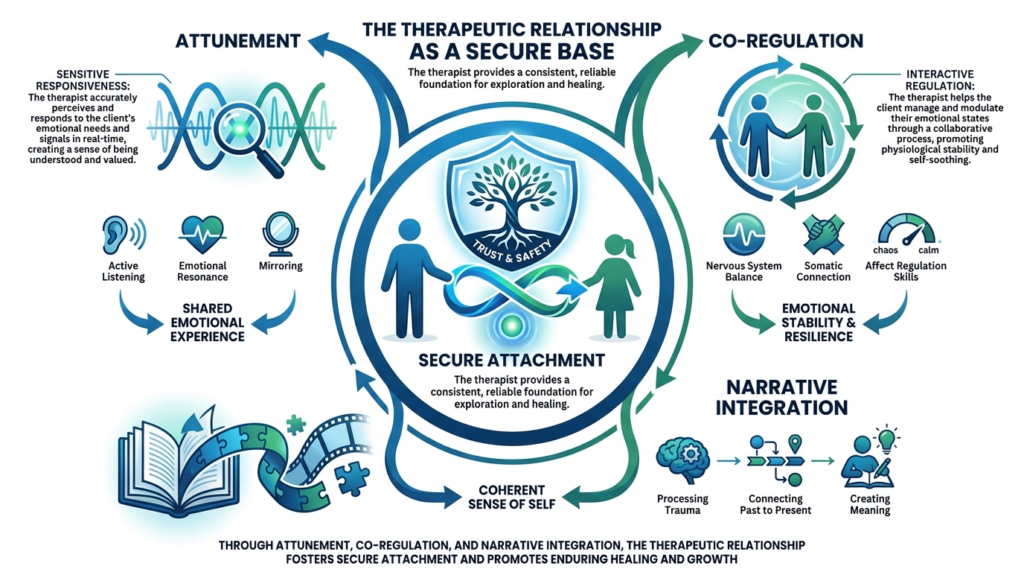
The Therapeutic Relationship as Mechanism
A key finding from recent attachment-trauma literature is that the therapeutic relationship is not just a supportive context. It is itself a corrective emotional and relational experience that models healthy, reliable interpersonal interaction. This aligns with updated trauma guidance emphasizing the therapeutic relationship as foundational to outcomes, especially in complex trauma.
For attachment trauma survivors, therapy often reactivates the very expectations it aims to heal: “You’ll leave,” “You’ll misunderstand me,” “If I need too much, you’ll reject me,” “If I trust you, I’ll get hurt,” “If I disagree, the relationship is over.” A therapist’s consistent attunement, boundaries, responsiveness, and repair can gradually disconfirm those expectations.
The 2025 clinical conceptualization specifically emphasizes ongoing monitoring of the therapeutic alliance, active repair of ruptures, and a cooperative, peer-based stance to reduce activation of traumatic internal working models.
For attachment trauma, rupture repair may be one of the central healing events. Many survivors have never had a conflict, misunderstanding, or disappointment successfully repaired within a close relationship. Therapy offers repeated opportunities to experience “something went wrong, and the relationship survived.”
Safety and Stabilization First
Phase-based trauma treatment literature reinforces that safety and stabilization are prerequisites for deeper processing. Phase-one guidance emphasizes physical, emotional, and relational safety, while warning against moving too quickly into trauma processing, neglecting alliance issues, or failing to assess readiness carefully.
This is particularly relevant for attachment trauma because the person may have limited self-regulation capacity, dissociation may interfere with processing, therapy itself may trigger attachment defenses, and memory processing without sufficient relational safety can destabilize rather than heal.
Evidence for Specific Therapeutic Approaches
Emotionally Focused Therapy
Emotionally Focused Therapy (EFT) is one of the clearest named attachment-based treatments in the evidence base.
According to the International Centre for Excellence in Emotionally Focused Therapy, EFT is grounded in adult attachment theory, meets high psychotherapy research standards, and is supported by meta-analytic findings. An older meta-analysis reported a large effect size of 1.3, and subsequent meta-analyses have confirmed efficacy.
EFT has evidence for changing relationship-specific attachment, may alter neural threat responding, and has positive findings for couples facing trauma, depression, and PTSD. A 2022 VA study of attachment-based couple treatment showed reductions in relationship distress, PTSD, and depressive symptoms.
Among named treatments in the supplied evidence, EFT has one of the strongest support profiles for relationally organized distress.
EMDR and Attachment-Focused Adaptations
EMDR is well-established for trauma, though the evidence specific to attachment trauma is more emerging than definitive. The strongest relevant item is a randomized controlled trial of 50 adolescents with bullying-related trauma comparing standard EMDR with attachment-based EMDR.
Both treatments reduced trauma and anxiety, but attachment-based EMDR produced faster, larger, and sustained improvements through two-month follow-up. The attachment-focused additions included self-compassion exercises, emotion regulation strategies, empathy training, and relational role-play alongside the standard eight-phase protocol.
This is a relatively small study focused on adolescent bullying trauma, so it should not be overgeneralized. But it provides concrete evidence that relationally targeted adjuncts may strengthen EMDR when trauma has significant attachment-linked features.
The evidence supports a careful opinion: EMDR appears useful for attachment trauma when adapted to include stabilization, resourcing, and explicit attention to relational safety and regulation, rather than being applied as a narrow protocol for isolated traumatic memories.
Attachment-Based Family Therapy
Attachment-Based Family Therapy (ABFT) is a specific, manual-guided, empirically supported treatment model grounded in attachment theory, developed particularly for adolescent depression, suicidality, and trauma. ABFT is structured around tasks including relational reframe, adolescent alliance, parent alliance, attachment task, and promoting competency and autonomy.
However, the 2024 systematic review and meta-analysis of ABFT for suicidal adolescents and young adults identified only 7 articles covering 4 randomized controlled trials (n = 287) and 3 open trials (n = 45).
In the randomized trials, ABFT was not significantly more effective than controls for suicidal ideation or depressive symptoms. The authors concluded that evidence is strongly limited by few available trials, small sample sizes, heterogeneity, attrition, and risk of bias.
ABFT is a legitimate, well-articulated, and clinically meaningful attachment-based family treatment, but as of 2026 its evidence for suicidal youth is promising yet inconclusive. It may work better for specific subgroups, particularly adolescents with higher baseline parent-teen conflict and underserved family backgrounds.
Dyadic Developmental Psychotherapy
Dyadic Developmental Psychotherapy (DDP) is a treatment approach for families of traumatized children or those with attachment-related difficulties, originally developed by Daniel Hughes.
It focuses on the parent-child relationship, attunement, emotional safety, co-regulation, and relational repair. DDP emphasizes therapist-parent-child attunement, a PACE/PLACE stance (playful, accepting, curious, empathic/loving), and co-construction of an alternative autobiographical narrative.
DDP materials explicitly state that restrictive, invasive, and constricting holds are not used. Where physical holding is referenced, it is described as non-restrictive cradling intended to support attunement, not coercive restraint.
This distinction matters because DDP is sometimes superficially associated with broader historical confusion around “attachment therapy.” Based on the supplied materials, DDP should be understood as a relational, attuned, non-coercive, dyadic therapy.
DDP appears conceptually coherent and clinically well-suited to complex developmental trauma in caregiver-child contexts, but within the supplied material its evidentiary presentation is less rigorous and more institution-driven than the ABFT evidence base.
What Actually Changes in Therapy?
Healing from attachment trauma involves several interconnected transformations.
From unsafety to relational safety. Attachment trauma teaches the person that closeness is dangerous, unreliable, engulfing, or futile. Therapy helps by providing a relationship that is bounded, consistent, and increasingly predictable.
This does not erase trauma history, but it begins to update procedural expectations. The person learns, over time, that needing, fearing, disagreeing, and being emotionally seen do not automatically lead to abandonment, humiliation, or chaos.
From dysregulation to co-regulation and self-regulation. Trauma-sensitive attachment-focused therapies aim not only to understand distress, but to regulate it. The person gradually becomes able to notice arousal, tolerate affect, reduce collapse or overwhelm, and use others in healthier ways for co-regulation.
From shame and pathogenic beliefs to healthier self-concept. Attachment trauma often generates beliefs such as “I am too much,” “I am unlovable,” “Others will hurt or abandon me,” “My needs are dangerous,” “I have to handle everything alone,” and “If I trust, I will be controlled or betrayed.” Recent clinical literature treats modification of these pathogenic beliefs as a core treatment target.
From dissociative fragmentation to integration. For many survivors, attachment trauma is not only about painful feelings but about disconnection from feelings, memory, body, and parts of self. Treatment helps reconnect these fragmented elements.
From mistrust to epistemic trust. Survivors of attachment trauma may not merely distrust people; they may distrust relationally transmitted knowledge. Advice, reassurance, perspective, and care may fail to “land.” Therapy helps by fostering epistemic trust gradually, so the person becomes more able to take in new relational experiences and revise old models.
Why Talk Therapy Alone Often Falls Short?
Trauma-sensitive, attachment-focused therapy is described as experiential rather than purely talk-based, aimed at healthy attachment and resilience, and addressing fear, shame, grief, and loss while enhancing emotional regulation and self-regulation skills.
The reason talk-based insight alone often falls short is straightforward: attachment trauma is encoded not just in narrative memory but in arousal patterns, implicit expectations, bodily states, dissociative responses, and procedural relationship templates.
A person may fully understand that their reactions come from childhood and still be unable to feel safe when someone gets emotionally close.
This does not mean cognitive or verbal approaches are useless. It means they are usually insufficient unless integrated with co-regulation, experiential work, emotion regulation training, attention to dissociation, relational repair, and processing of implicit memory and bodily activation.
Therapies treating attachment trauma as if it were mainly a mistaken belief system are likely to underperform, especially in patients with significant dissociation, relational panic, or chronic shutdown.
The strongest sources consistently indicate that safety, regulation, and relational experience are not optional add-ons; they are central mechanisms of change.
Practical Guidance for Recognizing Attachment Trauma
For individuals wondering whether attachment trauma applies to them, several signs may be relevant:
- You long for closeness but fear it
- You cannot trust support even when you want it
- Relationships repeatedly trigger panic, shutdown, or confusion
- You struggle with shame, emotional flooding, numbness, or detachment
- You understand your patterns intellectually but cannot shift them in real time
- Therapy helps temporarily but falls apart around trust, dependence, or rupture
These experiences do not prove attachment trauma, but they are consistent with it.
For clinicians, assessment should include childhood adversity, but also assess relational meaning, not just event count. Screen for dissociation, emotion regulation difficulties, attachment insecurity, and alliance sensitivity.
Watch for attachment trauma when treatment repeatedly stalls or destabilizes. Use phase-based stabilization when needed. Monitor and repair ruptures actively. Avoid rushing into trauma processing without sufficient safety and regulation capacity.
The Bottom Line on Attachment and Mental Health
Attachment trauma refers to chronic developmental trauma embedded in primary attachment relationships where caregiving repeatedly fails to provide protection, regulation, attunement, and safety, or becomes a source of ongoing abuse and threat.
Recent clinical scholarship has refined the concept and positioned it as a transdiagnostic framework with substantial relevance to dissociation, emotion dysregulation, mentalization deficits, pathogenic beliefs, epistemic mistrust, and treatment resistance.
Higher exposure to childhood adversity is linked to insecure adult attachment, especially patterns marked by fear of abandonment, avoidance of intimacy, problems with emotional closeness, and mistrust. Yet the most important findings go further: childhood adversity does not simply hardwire insecure attachment directly. Its effects are carried through mechanisms such as dissociation and emotion regulation difficulties.
Therapy helps when it addresses the actual architecture of the injury. The strongest cross-modality treatment principles are consistent: establish a safe therapeutic relationship, regulate emotions and arousal, repair alliance ruptures, modify pathogenic beliefs, address dissociated self-states, promote mentalization and epistemic trust, and process implicit and explicit traumatic memories.
Healing from attachment trauma is not simply remembering the past correctly. It is learning, often for the first time, that closeness can coexist with safety, that emotional states can be survived without collapse or abandonment, and that new relational experiences can revise old survival templates.
If you recognize these patterns in yourself or someone you care about, reaching out for help is a sign of strength, not weakness. At The Summit Wellness Group, we offer trauma-informed therapy that addresses the relational roots of emotional pain through evidence-based approaches including EMDR, attachment work, and somatic therapy in a compassionate, individualized setting.

