Many people struggling with trauma, anxiety, or addiction describe feeling at war with themselves. One part wants to heal, while another part resists change.
Internal Family Systems therapy offers a compassionate framework for understanding these inner conflicts. IFS proposes that the mind naturally contains multiple parts, each with protective intentions, and that healing occurs when these parts learn to trust a calm, centered Self.
This article explains what IFS therapy is, how it works in practice, and what current research reveals about its effectiveness.
What is Internal Family Systems Therapy?
Internal Family Systems is a psychotherapy model developed by Richard Schwartz in the 1980s while working as a family therapist. Schwartz noticed that clients spontaneously described their inner experience using language like “part of me wants this, but another part feels terrified.”
Rather than dismissing this as metaphor, he developed a structured approach that treats the mind as an internal system of subpersonalities organized around a core Self.
The model rests on a simple but powerful assumption: multiplicity is normal. Everyone has different parts that can become polarized after stress, attachment disruption, or trauma. Problems arise not because parts exist, but because they get pushed into extreme roles.
A pilot effectiveness study among survivors of multiple childhood trauma found that 16 sessions of IFS led to significant reductions in PTSD and depressive symptoms, with 92% of participants no longer meeting PTSD criteria at one month follow up.
IFS differs from traditional cognitive behavioral approaches by focusing on internal relationships rather than thought patterns alone.
Instead of challenging negative beliefs directly, therapists help clients develop curiosity toward the parts holding those beliefs. This shift from judgment to compassion often reduces shame and opens pathways for change.
The Core Components of IFS
Self: Your Internal Leader
At the center of IFS is the concept of Self, described as an undamaged core characterized by qualities like calm, curiosity, compassion, clarity, confidence, courage, creativity, and connectedness.
The Self is not a part but rather the person’s essence and natural internal leader. When someone accesses Self energy, they can relate to their parts with patience rather than criticism.
The therapeutic goal is not to eliminate parts but to help Self become the leading intelligence in the internal system.
This happens through a process therapists call unblending, where clients create enough space between their observing Self and an activated part so they are no longer completely engulfed by it.
The Three Types of Parts
IFS organizes parts into three categories based on their protective function:
Exiles carry pain, shame, terror, grief, or traumatic memories. These vulnerable parts often feel young and overwhelming. The internal system typically isolates them because their emotions feel too intense to handle. An exile might hold beliefs like “I am worthless” or “I will always be alone.”
Managers are proactive protectors that work to prevent exiled pain from surfacing. They control, organize, plan, and maintain performance. Perfectionism, people pleasing, harsh self criticism, and hypervigilance often reflect manager strategies. These parts believe that if they stay vigilant enough, nothing bad will happen.
Firefighters are reactive protectors that intervene when exiled pain breaks through despite the managers’ efforts. They use urgent strategies to extinguish emotional overwhelm, including numbing, impulsivity, rage, substance use, bingeing, or dissociation. While these behaviors may be harmful, the firefighter’s intent remains protective.
This framework helps clients understand that even destructive patterns serve a purpose. A 2013 study published in the Journal of Clinical Psychology argued that lack of self acceptance often blocks change, and that IFS builds acceptance of all parts, including destructive ones, to support transformation.
How IFS Therapy Works in Practice?
The Treatment Process
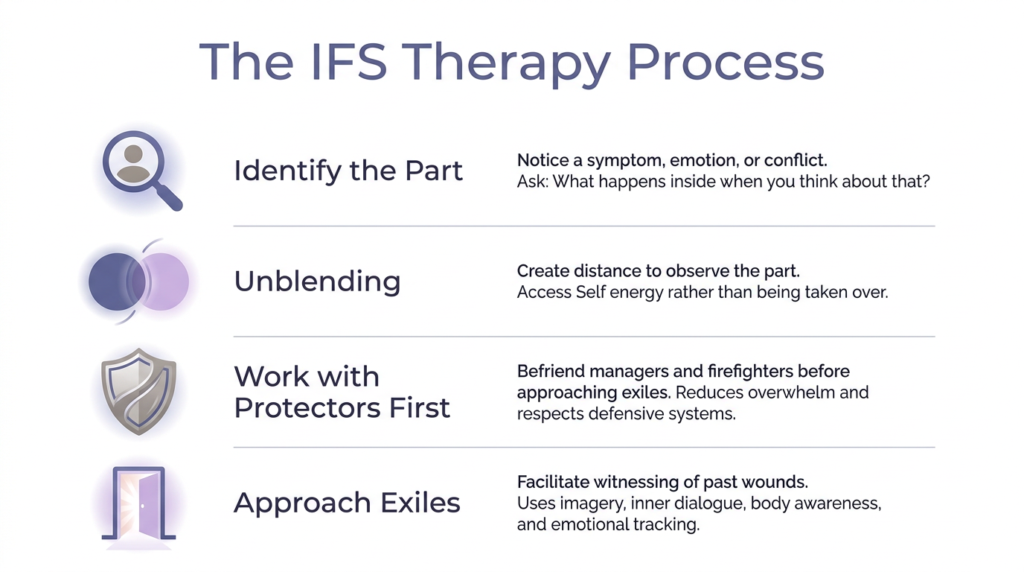
IFS therapy typically follows a recognizable sequence. First, the therapist helps clients identify a present symptom, emotion, or conflict and notice the part associated with it. The therapist might ask, “What happens inside when you think about that situation?” or “How do you feel toward that anxious part right now?”
Next comes unblending, where the client develops enough distance to observe the part rather than be completely taken over by it. If a client says “I hate this anxious part,” that hatred likely comes from another part. The therapist helps identify these layers until some Self energy becomes accessible.
IFS gives strong priority to befriending protectors before approaching vulnerable exiles. Training materials emphasize working with managers and firefighters first, especially in trauma work and high arousal states. This pacing reduces the risk of overwhelming clients and respects the wisdom of defensive systems.
Once protectors feel sufficiently understood and grant internal permission, therapy may shift toward exiles. The clinician facilitates witnessing of what happened, what the exile has carried, and what beliefs it took on. This process often involves imagery, inner dialogue, body focused noticing, and present moment emotional tracking.
A Clinical Example
Consider someone who freezes during work presentations and then attacks themselves afterward. An IFS therapist might identify a panic part, a critical manager, and beneath them an exiled part carrying old humiliation from being mocked in school.
The therapist would first help the client become curious about the critic rather than blended with it. Through dialogue, the critic might reveal it believes panic will lead to failure and social rejection. It attacks to force performance and prevent humiliation.
With more Self energy present, the client could contact the younger exiled part and witness that part’s fear and shame. As protective parts see the exile being attended to rather than exposed, they often relax. Over repeated sessions, panic and criticism become less extreme because the underlying shame is less isolated.
The Evidence Base for IFS
Current Research Status
The most responsible summary is that IFS has promising but limited evidence. It has moved beyond anecdotal support to include pilot studies and at least one randomized controlled trial, but the research base remains narrower than established trauma therapies like prolonged exposure, cognitive processing therapy, or EMDR.
A 2024 feasibility study published in Psychological Trauma examined an online group based IFS treatment for PTSD called the Program for Alleviating and Resolving Trauma and Stress. The study focused on whether participants could engage with and tolerate the intervention, finding encouraging results for attendance and satisfaction.
In 2026, researchers published the first randomized controlled trial of the PARTS program for PTSD. This milestone moved IFS into a new category of empirical support, though replication with larger samples is still needed.
The IFS Institute’s own research page acknowledges the evidence base is emerging and highlights a 2025 scoping review focused on current research, gaps, and future directions.
Conditions Where IFS Shows Promise
Public summaries commonly associate IFS with trauma, PTSD, complex trauma, anxiety, depression, addiction, eating disorders, and chronic pain. However, the quality of supporting evidence varies greatly across these conditions.
Some of the better known IFS evidence involves conditions outside PTSD. Psychology Today highlights a small randomized controlled trial in rheumatoid arthritis and a study on depression in young women. These suggest the model may be useful beyond trauma, though they do not justify broad claims about proven effectiveness across multiple psychiatric disorders.
For complex PTSD specifically, the evidence is notably thinner. Broader literature on cPTSD emphasizes phase based and multimodal treatment, heterogeneity of presentations, and the need to address disturbances in self organization beyond core PTSD symptoms.
A 2024 systematic review of interventions for trauma related dissociation identified 69 adult clinical studies, with IFS appearing in the peer reviewed trauma and dissociation conversation but only at an early stage.
Comparing IFS to Other Trauma Therapies
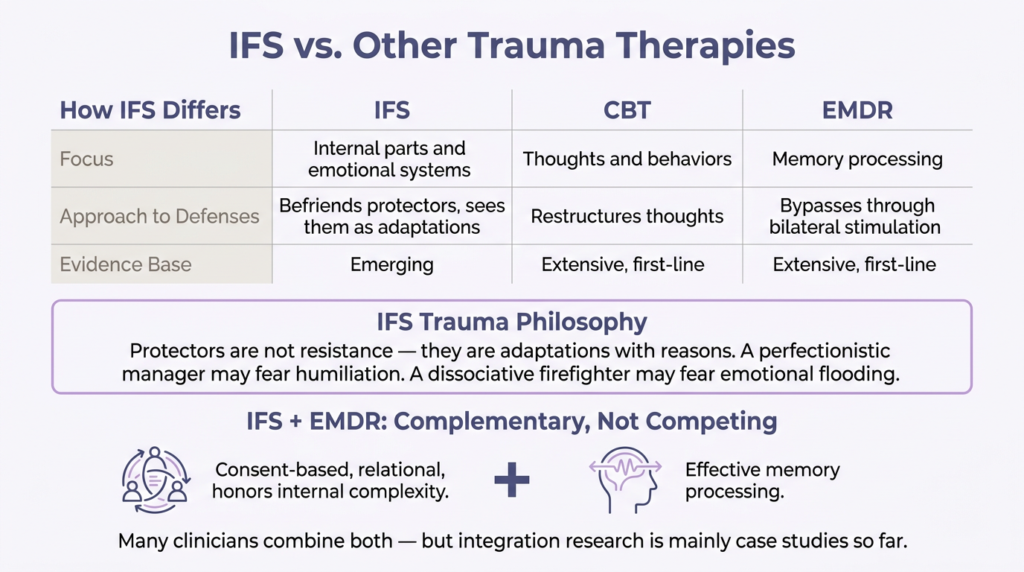
IFS differs from established trauma focused approaches in clinically meaningful ways. While cognitive behavioral therapy works primarily with thoughts and behaviors, and EMDR focuses on memory processing, IFS works with internal parts and emotional systems.
The model’s emphasis on befriending protectors before approaching traumatic material aligns with contemporary trauma informed values of pacing and consent. Rather than bypassing defenses as resistance, IFS understands them as adaptations with reasons. A perfectionistic manager may fear humiliation. A dissociative firefighter may fear emotional flooding.
However, IFS does not yet have the breadth of evidence supporting mainstream PTSD treatments. A 2019 guide to PTSD treatment guidelines explains that clinical practice guidelines typically prioritize randomized controlled trials, and that treatments like trauma focused CBT, cognitive processing therapy, prolonged exposure, and EMDR have large evidence bases and are generally recommended as first line options.
Many trauma clinicians do not treat IFS and EMDR as competitors. EMDRIA materials describe how IFS can complement EMDR by supporting a consent based, relational approach that honors internal complexity and helps clients tolerate processing more effectively. However, research on integrating the two approaches currently consists mainly of case studies.
Training and Certification Requirements
IFS can sound simple at the vocabulary level, but formal training is lengthy and structured. The IFS Institute offers progressive Level 1, Level 2, and Level 3 training, with certification as an additional process rather than automatic consequence of training completion.
For Certified Therapist status, applicants must hold an appropriate mental health degree, be licensed for clinical practice, complete Level 1 plus Level 2, document at least two years and 200 hours of post Level 1 regular IFS application, complete 15 hours of IFS continuing education and 15 hours of clinical consultation, obtain recommendation from an approved consultant, and pass a recorded or live session review.
The IFS certification policy explicitly states that certification does not expand professional scope of practice. Professionals must work only within the scope defined by their prior background. This warning is especially important for trauma, dissociation, and complex cases.
The IFS directory notes that some listed individuals may be practitioners in related fields rather than independently licensed therapists, and clients should confirm credentials. This distinction matters because IFS concepts have spread into coaching, spiritual counseling, bodywork, and other non clinical contexts.
Benefits and Limitations of IFS
Strengths of the Model
IFS offers several clinically valuable features. The “no bad parts” orientation can profoundly reduce shame for clients whose symptoms are entangled with moral self condemnation. By reframing troubling behaviors as protective efforts rather than defects, the model often helps people develop compassion toward themselves.
The framework gives structure to experiences many clients already report spontaneously: “part of me wants closeness but another part pushes people away” or “I know better but something takes over.” This mapping function is clinically useful even apart from full formal protocol use.
IFS emphasizes client led healing rather than therapist interpretation. The therapist guides but helps the client relate directly to parts. This can support agency and decrease dependency on expert decoding. Across public summaries of early studies, improvements in self compassion and emotional regulation recur frequently.
Important Limitations
The biggest limitation is straightforward: there are still relatively few high quality studies compared with older, better established psychotherapies. Even supportive sources acknowledge the research base is limited.
Healthline notes that because IFS emphasizes subpersonalities, it is generally not recommended for conditions like schizophrenia or dissociative identity disorder and may be unhelpful or destabilizing in some cases involving paranoia, confusion, or dissociation. The exact boundaries require clinical judgment, but the core point is valid: a parts based frame is not universally benign.
The same source mentions controversy involving malpractice allegations and the risk that a client’s “parts” might generate false traumatic memories under undue therapist pressure. This underscores the need for careful training, informed consent, non suggestive inquiry, attention to memory science, and strong trauma ethics.
Variable practitioner training also matters. Because many therapists use IFS informed language with differing training depth, treatment quality may vary considerably. The difference between “IFS informed,” “trained in IFS,” and “IFS certified therapist” is clinically important.
Who is Most Likely to Benefit?
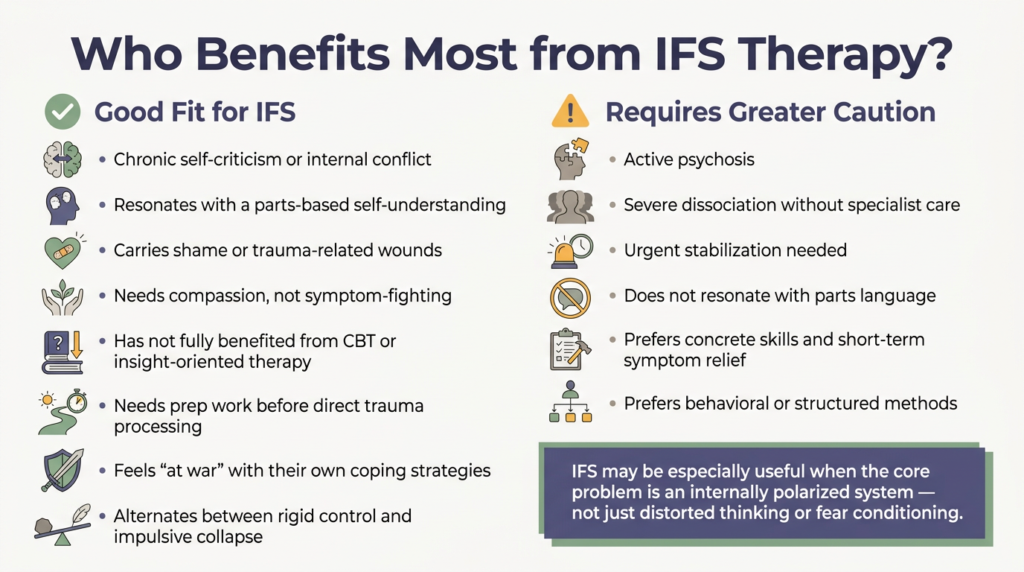
Based on current evidence and clinical descriptions, IFS is most likely to be a good fit for people who experience chronic self criticism or internal conflict, resonate with a parts based understanding of themselves, carry shame or trauma related wounds, need a compassionate framework rather than symptom fighting, have not fully benefited from more cognitive or purely insight oriented therapies, or need preparatory work before more direct trauma processing.
The model may be especially useful when the main problem is not simply distorted thinking or fear conditioning, but an internally polarized system. For example, someone who alternates between rigid control and impulsive collapse, or who feels “at war” with their own coping strategies, may find IFS particularly clarifying.
By contrast, IFS may require greater caution when psychosis is active, severe dissociation is present without specialist care, urgent stabilization is needed, or the client does not resonate with internal parts language. Some people prefer concrete skills, strong structure, short term symptom relief, or more straightforward behavioral methods.
The Bottom Line on IFS Therapy
Internal Family Systems is a legitimate and potentially powerful psychotherapy model, especially for trauma related inner conflict and self relational healing. It deserves serious consideration as an emerging trauma psychotherapy. However, its public reputation currently exceeds the breadth and strength of its empirical support.
The most accurate current position is that IFS is an emerging evidence based approach rather than a gold standard first line therapy across diagnoses. It has crossed an important threshold by producing a first PTSD randomized controlled trial, but it still lacks the depth, replication, comparative breadth, and guideline level integration needed to justify the strongest public claims often made on its behalf.
For clinicians, this means representing evidence honestly, clarifying training level, using trauma pacing carefully, avoiding overgeneralizing from group based studies, and being cautious in severe psychosis or severe identity fragmentation contexts.
For potential clients, it means understanding that IFS is a real psychotherapy model with genuine clinical value, but that the skill of the therapist matters greatly, especially in trauma work.
If you are struggling with trauma, addiction, or co-occurring mental health conditions and want to explore whether IFS or other evidence based therapies might help, consider reaching out to The Summit Wellness Group because we offer comprehensive, individualized care. Contact our team to learn more about trauma informed treatment options.

