Sleeping too much when you’re depressed isn’t laziness or weakness. It’s a real symptom that affects roughly one in four people with major depression and can make recovery harder.
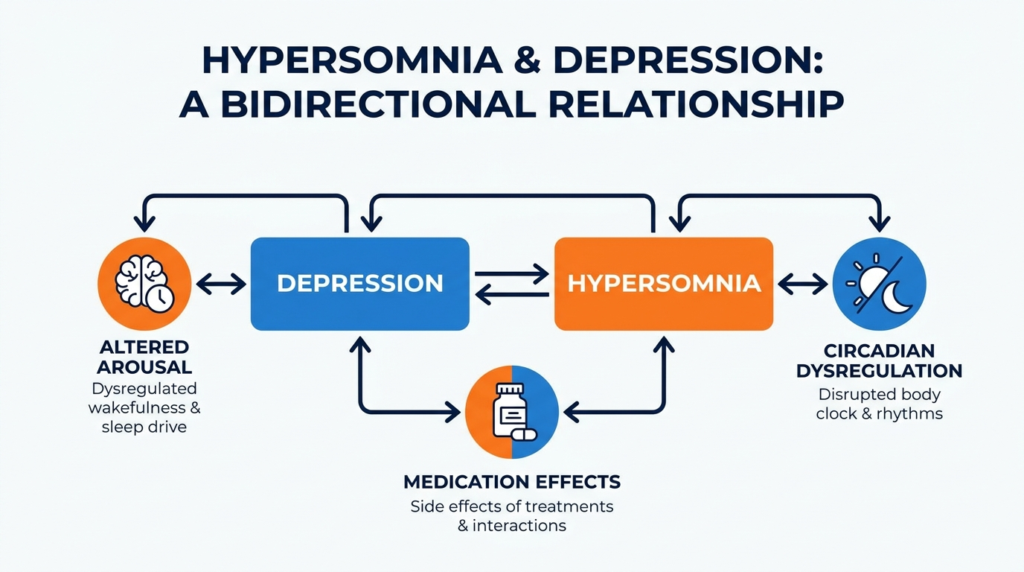
Depression can cause hypersomnia through disrupted brain chemistry, circadian rhythm problems, and changes in how your body regulates wakefulness, though the full picture often includes medication effects, sleep disorders like sleep apnea, or behavioral withdrawal.
This article explains what connects depression and excessive sleepiness, how to tell if your oversleeping is part of depression or something else, and what treatment options actually help.
What is Hypersomnia in Depression?
Hypersomnia in depression means more than just feeling tired. It’s a pattern of excessive daytime sleepiness, prolonged nighttime sleep, or spending too much time in bed that happens alongside depressive symptoms. The term can be confusing because it’s used in different ways.
Sleep medicine defines excessive daytime sleepiness as difficulty staying awake during the day, often leading to unintended naps. In psychiatric settings, hypersomnia might instead describe sleeping longer than usual, difficulty waking up, or simply spending more hours in bed.
This distinction matters because a patient who says “I sleep 12 hours” might actually mean they’re lying in bed that long, not necessarily sleeping the entire time. Research shows that in mood disorders, subjective reports of long sleep often don’t match objective measurements. Many depressed patients feel profoundly sleepy or unable to get going, yet sleep studies show normal sleep duration and normal daytime sleep propensity.
That mismatch doesn’t mean the symptom is imaginary. It suggests depression-related hypersomnia involves altered wake drive, nonrestorative sleep, motivational slowing, or increased time in bed rather than classic physiologic sleepiness alone.
The practical takeaway is that clinicians should distinguish sleepiness from fatigue, low energy, and insufficient sleep, because these overlapping complaints have different causes and treatments.
How Common is Hypersomnia in Depression?
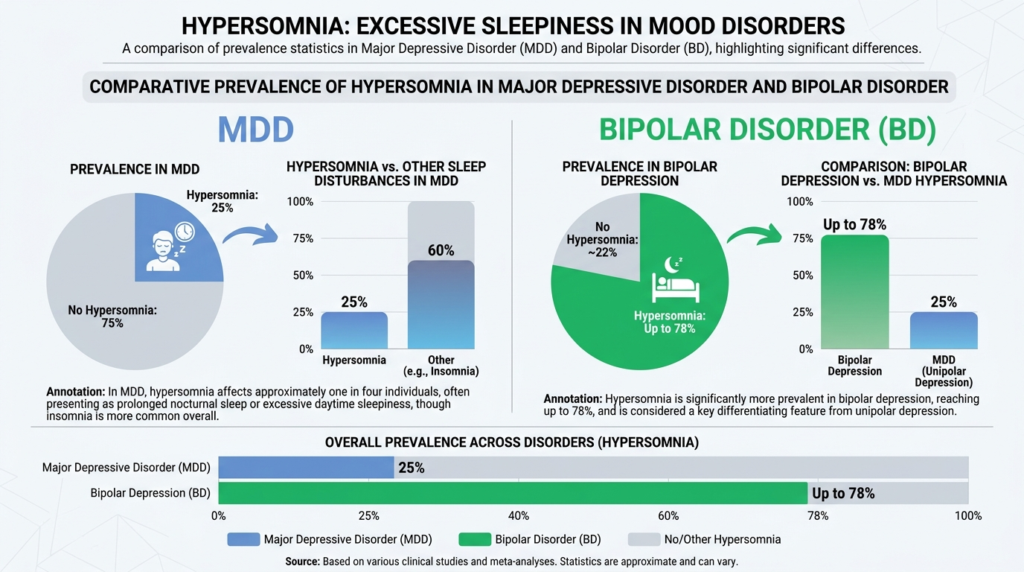
Hypersomnia affects about 25% of patients with major depressive disorder, though it’s often overlooked in routine clinical practice despite its effect on remission and quality of life. Other reviews place the prevalence closer to 30% of individuals with MDD and note associations with longer, more severe, and more treatment-resistant depressive episodes.
In bipolar disorder, hypersomnia is even more prominent. A recent review found that while insomnia was more common overall at 43%, hypersomnia was also frequent at 29%, and both were more common than having no sleep problems. In bipolar depression specifically, hypersomnia prevalence estimates range from 38% to 78% and it’s described as highly recurrent.
Notably, 35% of euthymic individuals with bipolar I disorder endorsed hypersomnia, suggesting that oversleeping isn’t purely an episode-bound symptom but may reflect a more stable vulnerability.
The relationship appears bidirectional. Prospective studies suggest that people with hypersomnia are about 2.4 to 2.9 times more likely to later develop a depressive episode. This means hypersomnia isn’t only a consequence of depression; it may also be a marker of vulnerability or an early phase in the development of future depressive illness.
Can Depression Cause Hypersomnia?
Yes, depression can cause hypersomnia symptoms and often does. This is best established for subjective hypersomnolence, oversleeping, difficulty awakening, and increased daytime napping or sleep desire. However, depression-associated hypersomnia often lacks the objective sleep test abnormalities that characterize central hypersomnolence disorders like narcolepsy or idiopathic hypersomnia.
Several lines of evidence support a causal contribution of depression to hypersomnia. First, hypersomnia is a recognized symptom in depressive illness, particularly in atypical depression and seasonal forms. Atypical depressive episodes commonly present with hypersomnia, increased appetite, weight gain, mood reactivity, leaden paralysis, and rejection sensitivity.
Second, large proportions of patients with major depression and bipolar depression report hypersomnolence or oversleeping, far above general population rates. Third, hypersomnia may persist even as mood partially improves, implying it’s not merely incidental background distress.
The causal statement needs qualification for two reasons. First, the symptom may not be purely caused by depression. Psychiatric patients often have multiple coexisting contributors including obesity, obstructive sleep apnea, sedative medications, disrupted routines, and circadian dysregulation.
Reviews explicitly caution clinicians to consider iatrogenic causes and sleep apnea syndrome, especially because psychiatric patients are often overweight and prescribed sedative drugs.
Second, many depressed patients with hypersomnolence don’t demonstrate objective daytime sleepiness on the Multiple Sleep Latency Test. This means depression often causes a syndrome of “feeling excessively sleepy” that isn’t identical to narcolepsy-like physiologic sleep propensity.
Depression can cause clinically significant hypersomnia symptoms, but these symptoms frequently reflect a subjective and multifactorial disturbance of arousal, sleep quality, circadian regulation, and behavior rather than a pure central hypersomnolence disorder.
Why Does Depression Lead to Hypersomnia?
The literature doesn’t identify one definitive cause for hypersomnolence in depression. Instead, the best-supported model is multifactorial, involving interacting biological, circadian, behavioral, and treatment-related pathways.
Altered Arousal and Wake Drive
Several reviews suggest that hypersomnolence in mood disorders may arise from impaired wake drive rather than simply too much sleep.
Recommendations to avoid sedating psychotropics and preferentially use noradrenergic antidepressants when possible reflect the view that enhancing catecholaminergic tone may improve wakefulness.
The relative benefit of bupropion over SSRIs for residual sleepiness further supports involvement of dopamine and norepinephrine systems.
Circadian Dysregulation
Depression frequently involves disrupted biological rhythms. The chronotherapy literature proposes that interventions targeting sleep timing, total sleep deprivation, and bright light can rapidly shift mood and wakefulness, suggesting that at least some depressive hypersomnia is driven by circadian misalignment or instability.
Clinical considerations around delayed sleep phase syndrome are especially relevant in patients whose chief complaints are morning sleepiness and difficulty awakening rather than all-day sleep propensity.
Nonrestorative Sleep
Some review discussions suggest that depressive hypersomnolence may be linked to impaired sleep homeostasis or altered slow-wave activity dynamics.
The observation that mirtazapine may improve sleepiness while enhancing slow-wave sleep, without necessarily increasing total sleep time, is consistent with the idea that “quality” or restorative value of sleep may matter as much as quantity.
Behavioral Withdrawal
Patients with depression may spend more time in bed, nap more, withdraw from activities, and reduce daytime stimulation.
Some sources note that patients may be “resting” more than actually sleeping. This can perpetuate inertia, worsen sleep fragmentation, and intensify the subjective sense of hypersomnia.
Medication-Induced Somnolence
A major confound is treatment itself. SSRIs are associated with higher rates of somnolence than placebo and bupropion, and antidepressant-related sedation can resemble or worsen primary hypersomnolence complaints.
Benzodiazepines and hypnotics can also create next-day sedation and “hangover” effects, so eliminating unnecessary sedating agents is a core management principle.
Comorbid Sleep Disorders
Obstructive sleep apnea, restless legs syndrome, circadian rhythm sleep-wake disorders, and narcolepsy or idiopathic hypersomnia can all coexist with depression and amplify sleepiness.
This is particularly important because untreated sleep apnea may produce both depressive symptoms and excessive daytime sleepiness, making causality appear more psychiatric than it is.
Symptoms of Hypersomnia in Depression
Depression-related hypersomnia is more than “sleeping too much.” Clinical presentation typically includes a cluster of subjective complaints and behavioral patterns.
Common symptoms include prolonged nocturnal sleep duration, excessive daytime sleepiness, frequent or prolonged daytime naps, difficulty awakening at the desired time, sleep inertia or “sleep drunkenness,” unrefreshing sleep, low energy that patients may describe as sleepiness, spending excessive time in bed, and impaired concentration and psychomotor slowing.
Fatigue is one of the main reasons hypersomnia is under- or misdiagnosed. Clinical reviews note that patients may identify their problem as being “tired,” “run down,” or “low energy,” but these phrases are nonspecific and may reflect pain, disability, depression, or true sleepiness.
A depressed patient may sincerely believe they’re sleepy when the predominant issue is fatigue, or the opposite may occur.
Key Symptom Patterns
- Prolonged sleep: Sleeping 9 to 12 hours or more per night
- Daytime sleepiness: Dozing off unintentionally or feeling irresistibly sleepy
- Unrefreshing sleep: Waking up feeling exhausted despite long sleep
- Difficulty waking: Severe grogginess, inability to get out of bed
- Excessive napping: Taking long naps that don’t restore energy
- Time in bed: Spending hours lying in bed without necessarily sleeping
Is Hypersomnia a Symptom of Depression?
Yes, hypersomnia is a recognized symptom of depression, particularly in atypical depression and seasonal affective disorder. It appears in diagnostic criteria and is commonly reported by patients with major depressive disorder and bipolar depression. However, calling it “a symptom of depression” can be misleading if it suggests the problem is purely psychiatric or will automatically resolve when mood improves.
Hypersomnia in depression is clinically serious. It’s associated with resistance to treatment, relapse, suicidality risk, and impaired functioning. Review literature citing STAR*D data notes that hypersomnia may fail to improve during citalopram treatment in non-remitters.
One major review explicitly identifies hypersomnia in mood disorders as associated with increased risk of suicide, underscoring that clinicians shouldn’t trivialize the symptom as merely inconvenient or “behavioral.”
Daytime sleepiness, prolonged sleep, and difficult awakening can damage occupational performance, school functioning, driving safety, social participation, and adherence to therapy. This impairment often persists even when mood partially improves. Because hypersomnia may signal sleep apnea or medication toxicity, failing to evaluate it thoroughly can allow treatable contributors to persist.
When Hypersomnia Isn’t Just Depression?
The differential diagnosis is where psychiatry and sleep medicine connect most usefully. The best evidence-based approach isn’t to choose between “depression” and “sleep disorder,” but to actively consider both.
Obstructive Sleep Apnea
Sleep apnea is one of the most important alternative or coexisting diagnoses. A 2023 Delphi consensus noted that excessive daytime sleepiness is common in sleep apnea and can persist even after primary airway therapy is optimized.
In an apneic cohort study, the prevalence of major depressive disorder was 26.3%, and excessive daytime sleepiness in apneic individuals was associated with a higher likelihood of depression.
This has two major implications. Depression can coexist with sleep apnea and magnify sleepiness, and sleep apnea-associated excessive daytime sleepiness may contribute to or worsen depressive syndromes.
Any depressed patient with hypersomnia, obesity, snoring, or nonrestorative sleep should be evaluated for sleep apnea early rather than after multiple failed antidepressant trials.
Medication-Induced Hypersomnolence
Sedative psychotropics, benzodiazepines, hypnotics, some antipsychotics, and certain antidepressants can all worsen hypersomnolence.
Reviews specifically recommend a careful chronology of prescribed and over-the-counter medications whenever hypersomnia is evaluated. The mood disorder literature echoes this concern and specifically advises avoiding benzodiazepines when possible in depressed patients with hypersomnia.
Narcolepsy and Idiopathic Hypersomnia
Primary central hypersomnolence disorders should be considered especially when sleepiness predates mood symptoms, naps are irresistible or restorative, cataplexy is present, sleep-onset REM periods are documented, or the Multiple Sleep Latency Test shows short sleep latencies. Narcolepsy is differentiated by excessive daytime sleepiness, cataplexy, and two or more sleep-onset REM periods on MSLT.
However, one of the major challenges is that psychiatric comorbidity is also common in central hypersomnia disorders, making the distinction genuinely difficult rather than merely procedural.
Circadian Rhythm Sleep-Wake Disorders
Delayed sleep-wake phase disorder can mimic hypersomnia when the real problem is severe morning sleepiness and difficulty awakening, with preserved alertness later in the day.
This is especially relevant in younger adults, evening chronotypes, and individuals with irregular schedules.
Insufficient Sleep
Behaviorally induced insufficient sleep syndrome remains a common cause of excessive daytime sleepiness and should be excluded before attributing symptoms to depression or central hypersomnolence.
Many depressed patients have fragmented sleep, inconsistent schedules, or compensatory oversleeping that masks a fundamentally poor sleep-wake routine.
How to Assess Hypersomnia in Depression?
Clinicians should begin by distinguishing sleepiness, fatigue, low motivation, time in bed, long sleep duration, naps, and difficulty awakening. Subjective self-report can identify problems but is often unreliable or imprecise.
The most useful early question is often: Did the hypersomnia precede, accompany, or follow the depressive symptoms? This chronology is specifically recommended in differential diagnosis sources and can separate primary hypersomnia from secondary depressive hypersomnolence.
Minimum evaluation should include medication review, sleep schedule review, snoring and apnea screening, body weight and BMI context, substance use, restless legs symptoms, shift work or delayed phase, bipolar symptoms, cataplexy or sleep paralysis, and driving safety risk.
The Epworth Sleepiness Scale is widely used and was the measure for excessive daytime sleepiness in the cited sleep apnea cohort, where EDS was defined as ESS greater than 10. However, scale scores shouldn’t substitute for careful clinical assessment.
Polysomnography and the Multiple Sleep Latency Test should be considered when symptoms suggest another sleep disorder, particularly sleep apnea, narcolepsy, or idiopathic hypersomnia.
However, clinicians should recognize that in depression these tests are often normal despite marked complaints. Actigraphy can help objectively assess sleep patterns and circadian rest-activity rhythms in patients with depression.
Treatment Options for Depression and Hypersomnia
Treatment of depression-related hypersomnia is one of the weakest areas in the evidence base, but several practical conclusions emerge.
Treat the Depression, But Don’t Assume Hypersomnia Will Resolve
A recurrent finding is that hypersomnia may persist even when other depressive symptoms improve. Review literature citing STAR*D data notes that hypersomnia may fail to improve during citalopram treatment in non-remitters. Therefore, “let’s just treat the depression and wait” is often insufficient.
Remove Iatrogenic Contributors
This is the most consistently supported first-line step: reduce or avoid benzodiazepines when possible, minimize hypnotic “hangover” effects, reassess sedating antidepressants and antipsychotics, consider medication timing, and avoid unnecessary sedative substances.
Consider Antidepressant Selection Based on Wakefulness Profile
Evidence suggests that bupropion is associated with fewer residual sleepiness symptoms than SSRIs among remitted patients, despite similar depression remission rates.
A recent review states that SSRIs alone may be insufficient, and that noradrenaline and dopamine reuptake inhibitors or similar agents are generally indicated.This is one of the most actionable findings in the literature. If a depressed patient is hypersomnolent on an SSRI and no contraindication exists, a more activating antidepressant strategy may be preferable.
SSRIs are effective antidepressants but are associated with higher rates of somnolence than placebo and bupropion in meta-analytic data.
Paradoxically, a small study found that the sedating antidepressant mirtazapine improved daytime sleepiness and fatigue in depressed patients on both subjective measures and the Multiple Sleep Latency Test, possibly by enhancing slow-wave sleep quality rather than by increasing overall sedation burden.
This finding is intriguing but should be interpreted cautiously because the evidence base is small and mirtazapine can also cause daytime sedation and weight gain in many patients.
Wake-Promoting Agents for Residual Hypersomnia
There are no medications specifically approved for hypersomnia in mood disorders, but modafinil and armodafinil are the most studied adjunctive agents for residual fatigue and sleepiness in unipolar and bipolar depression.
Their use is extrapolated from both depression augmentation trials and their approved indications in narcolepsy, sleep apnea-related residual sleepiness, and shift-work disorder.
Advantages include being the best-studied wake-promoting adjuncts in mood disorders and may help when residual sleepiness persists despite antidepressant or mood-stabilizing treatment.
Limitations include being off-label for mood-disorder hypersomnia, may not address underlying depression if that remains inadequately treated, and stimulant-like strategies in bipolar disorder require caution because of possible affective switching.
Bright Light Therapy and Chronotherapeutics
A pragmatic randomized controlled trial evaluated total sleep deprivation followed by bright light therapy as a rapid-relief strategy for depression, supporting chronotherapeutics as a potentially fast-acting option.
The same paper notes that repeated total sleep deprivation and standardized sleep management protocols may matter, light parameters may influence efficacy, and potential predictors of better response include bipolar disorder, lower anxiety, prior antidepressant response, positive diurnal mood variation, and evening chronotype, though these require validation.
For depression with hypersomnia, bright light therapy is attractive because it may advance circadian timing, improve morning alertness, reduce depressive symptoms, and support wake drive without adding sedative burden.
Cognitive and Behavioral Interventions
The 2024 review on depression-associated hypersomnolence identifies CBT for hypersomnia as an emerging adjunctive treatment. This is important because standard depression therapy often doesn’t directly target prolonged sleep, time in bed, or dysfunctional beliefs about sleepiness.
General excessive daytime sleepiness management guidance recommends regular schedules, standing and movement to improve alertness, caffeine strategically earlier in the day, bright light exposure, removing sedative substances, and chronotherapeutic adjustment of medication timing. These measures are low-risk and often useful, though they’re adjunctive rather than definitive.
Treat Coexisting Sleep Disorders Directly
If sleep apnea is present, airway therapy is essential. The Delphi consensus on excessive daytime sleepiness in sleep apnea highlights that sleepiness may persist even after optimizing primary treatment, which means post-CPAP residual sleepiness still requires evaluation rather than dismissal.
In apneic individuals, because excessive daytime sleepiness is associated with major depressive disorder, addressing sleepiness may help depressive symptom burden as well.
When to Seek Professional Help?
You should seek professional evaluation if you experience persistent hypersomnia alongside depressive symptoms, especially if you notice difficulty waking despite long sleep, unrefreshing sleep that leaves you exhausted, daytime sleepiness that interferes with work or safety, snoring or witnessed breathing pauses during sleep, hypersomnia that persists despite depression treatment, or sudden worsening of sleepiness after medication changes.
Professional assessment becomes urgent if hypersomnia is accompanied by suicidal thoughts, severe functional impairment, or symptoms suggesting narcolepsy such as sudden muscle weakness triggered by emotion or vivid hallucinations when falling asleep or waking.
If you’re struggling with depression and excessive sleepiness that won’t improve, our comprehensive evaluation can identify treatable causes and guide effective treatment. Contact our team to discuss how integrated mental health and sleep-focused care can help you reclaim your energy and well-being.

